

Age-Based Causes and Clinical Characteristics of Immediate-Type Food Allergy in Korean Children
- PMID: 28677356
- PMCID: PMC5500697
- DOI: 10.4168/aair.2017.9.5.423
Age-Based Causes and Clinical Characteristics of Immediate-Type Food Allergy in Korean Children
Abstract
Purpose: Age-based causes and clinical characteristics of immediate-type food allergy (FA) have not been sufficiently studied. Therefore, we investigated age-dependent clinical profiles of FA in Korean children through an extensive multicenter investigation.
Methods: Using a case report form developed by the authors, a retrospective medical record review was performed of patients (0-18 years old) diagnosed with immediate-type FA between September 2014 and August 2015 in 14 tertiary hospitals in Korea.
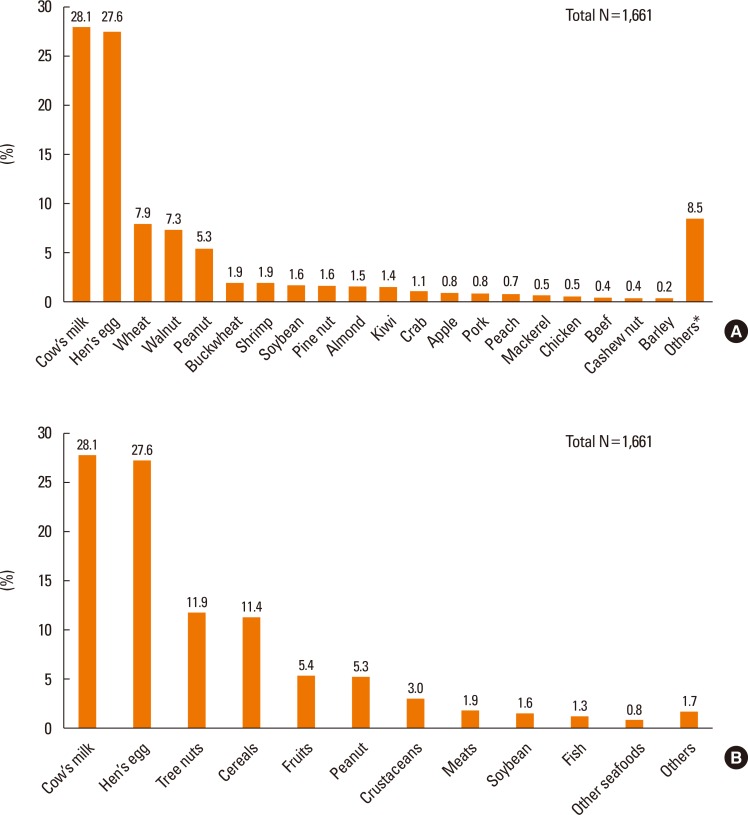
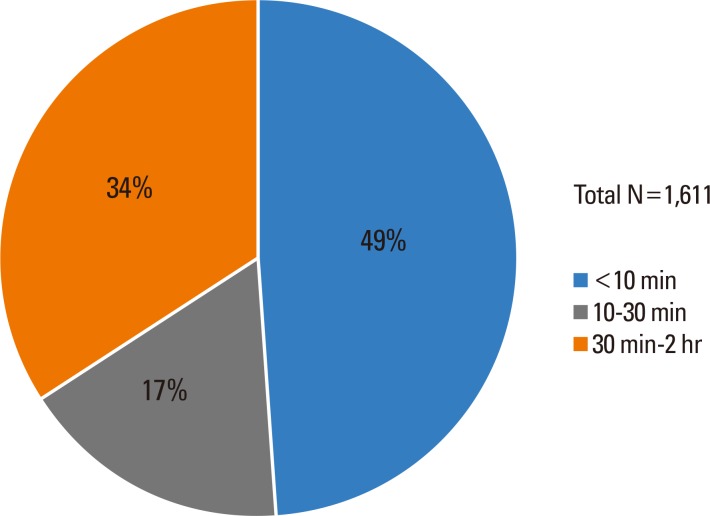
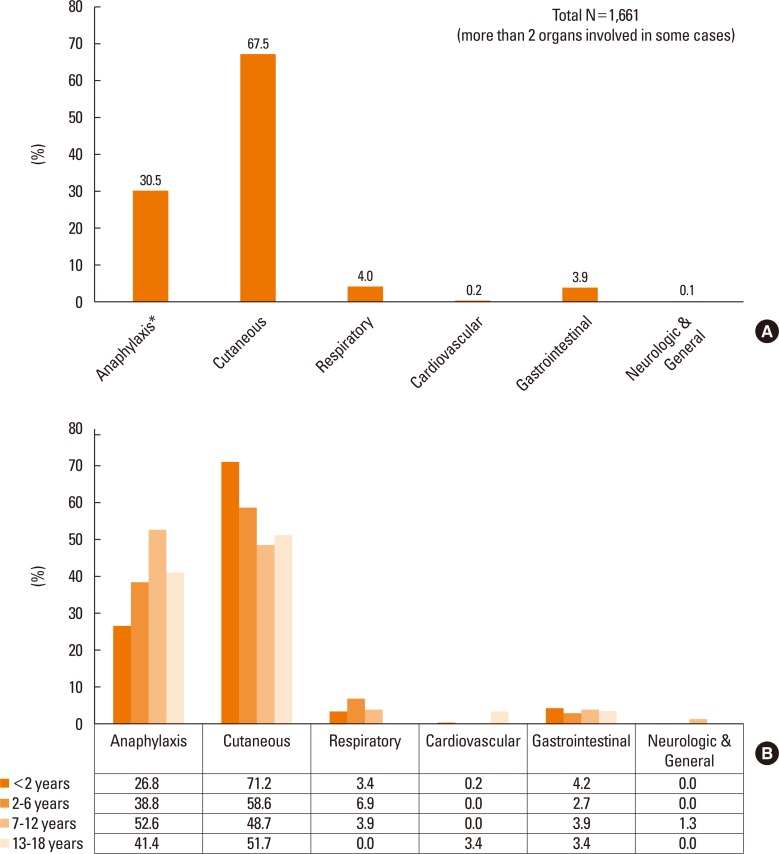
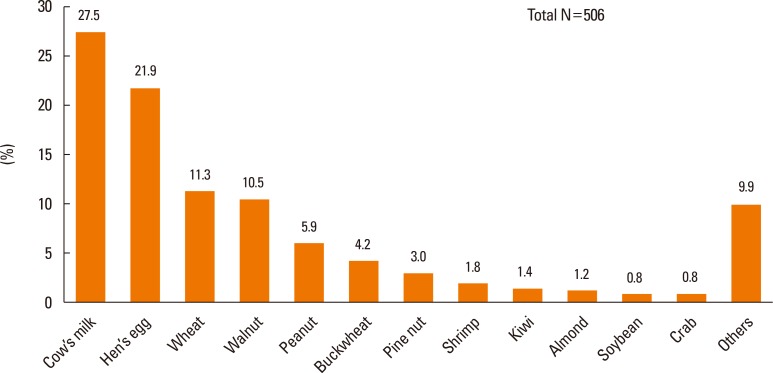
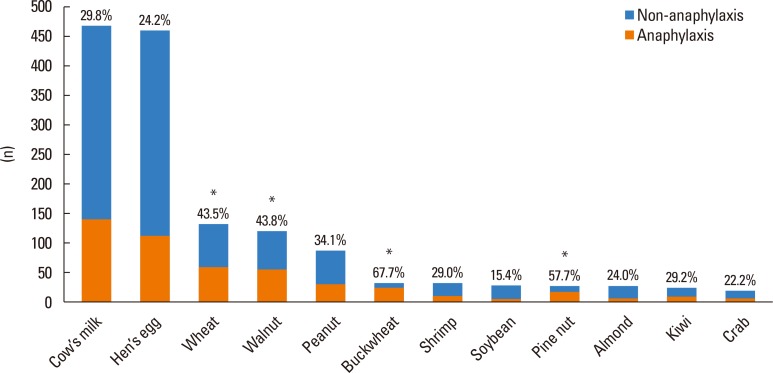
Results: A total of 1,353 children and adolescents, 93% younger than 7 years, were enrolled in the present study, and 1,661 cases of immediate-type FA were recorded in these patients. The 7 major causative foods were cow's milk (28.1%), hen's eggs (27.6%), wheat (7.9%), walnuts (7.3%), peanuts (5.3%), buckwheat (1.9%), and shrimps (1.9%). Categorizing the patients into 4 age groups revealed that the most common causative food was different for each age group: cow's milk (<2 years), walnuts (2-6 years), walnuts (7-12 years), and buckwheat (13-18 years). The onset time of symptoms was less than 10 minutes in 49%, between 10 and 30 minutes in 17%, and between 30 minutes and 2 hours in 34% of cases. Food-induced anaphylaxis was reported in 506 (30.5%) out of 1,661 cases, and the 7 major causes of food-induced anaphylaxis was cow's milk (27.5%), hen's eggs (21.9%), wheat (11.3%), walnuts (10.5%), peanuts (5.9%), buckwheat (4.2%), and pine nuts (3.0%). The proportion of anaphylaxis was highest in the patients allergic to buckwheat (67.7%), followed by those allergic to pine nuts (57.7%), walnuts (43.8%), wheat (43.5%), and peanuts (34.1%).
Conclusions: The 5 major causative foods of immediate-type FA in Korean children were cow's milk, hen's eggs, wheat, walnuts, and peanuts. The distribution of causative foods was considerably distinctive according to different age groups. Anaphylaxis was reported in 30.5% of immediate-type FA cases.
Keywords: Food hypersensitivity; IgE-mediated; adolescents; anaphylaxis; children.
Copyright © 2017 The Korean Academy of Asthma, Allergy and Clinical Immunology · The Korean Academy of Pediatric Allergy and Respiratory Disease
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interest.
Figures
Similar articles
-
Prevalence of Immediate-Type Food Allergy in Korean Schoolchildren in 2015: A Nationwide, Population-based Study.Allergy Asthma Immunol Res. 2017 Sep;9(5):410-416. doi: 10.4168/aair.2017.9.5.410. Allergy Asthma Immunol Res. 2017. PMID: 28677354 Free PMC article.
-
Infantile Anaphylaxis in Korea: a Multicenter Retrospective Case Study.J Korean Med Sci. 2019 Apr 8;34(13):e106. doi: 10.3346/jkms.2019.34.e106. J Korean Med Sci. 2019. PMID: 30950251 Free PMC article.
-
Prevalence of immediate-type food allergy in early childhood in seoul.Allergy Asthma Immunol Res. 2014 Mar;6(2):131-6. doi: 10.4168/aair.2014.6.2.131. Epub 2013 Nov 28. Allergy Asthma Immunol Res. 2014. PMID: 24587949 Free PMC article.
-
Timing of Food Introduction and the Risk of Food Allergy.Nutrients. 2019 May 21;11(5):1131. doi: 10.3390/nu11051131. Nutrients. 2019. PMID: 31117223 Free PMC article. Review.
-
Chapter 23: Food allergy.Allergy Asthma Proc. 2012 May-Jun;33 Suppl 1:77-79. doi: 10.2500/aap.2012.33.3556. Allergy Asthma Proc. 2012. PMID: 22794696 Review.
Cited by
-
Food allergy and food-induced anaphylaxis in children: an increasing critical public health issue.Korean J Pediatr. 2019 Dec;62(12):431-432. doi: 10.3345/kjp.2019.00493. Epub 2019 Nov 12. Korean J Pediatr. 2019. PMID: 31870083 Free PMC article. No abstract available.
-
Recent advances in food allergen immunotherapy.Clin Exp Pediatr. 2024 Aug;67(8):386-394. doi: 10.3345/cep.2023.01004. Epub 2023 Dec 7. Clin Exp Pediatr. 2024. PMID: 38062712 Free PMC article.
-
Asia Pacific Allergy: A great platform for allergy.Asia Pac Allergy. 2018 Oct 30;8(4):e42. doi: 10.5415/apallergy.2018.8.e42. eCollection 2018 Oct. Asia Pac Allergy. 2018. PMID: 30402409 Free PMC article. No abstract available.
-
Combined Effects of Lactobacillus rhamnosus and Egg Oral Immunotherapy in a Mouse Model of Egg Allergy.Allergy Asthma Immunol Res. 2020 Jul;12(4):701-711. doi: 10.4168/aair.2020.12.4.701. Allergy Asthma Immunol Res. 2020. PMID: 32400134 Free PMC article.
-
Milk-Related Symptoms and Immunoglobulin E Reactivity in Swedish Children from Early Life to Adolescence.Nutrients. 2018 May 21;10(5):651. doi: 10.3390/nu10050651. Nutrients. 2018. PMID: 29883392 Free PMC article.
References
-
- Longo G, Berti I, Burks AW, Krauss B, Barbi E. IgE-mediated food allergy in children. Lancet. 2013;382:1656–1664. - PubMed
-
- Sánchez-García S, Cipriani F, Ricci G. Food allergy in childhood: phenotypes, prevention and treatment. Pediatr Allergy Immunol. 2015;26:711–720. - PubMed
-
- Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics. 2011;128:e9–e17. - PubMed
-
- Rona RJ, Keil T, Summers C, Gislason D, Zuidmeer L, Sodergren E, et al. The prevalence of food allergy: a meta-analysis. J Allergy Clin Immunol. 2007;120:638–646. - PubMed
-
- Soller L, Ben-Shoshan M, Harrington DW, Fragapane J, Joseph L, St Pierre Y, et al. Overall prevalence of self-reported food allergy in Canada. J Allergy Clin Immunol. 2012;130:986–988. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
