

Long-term health status and trajectories of seriously injured patients: A population-based longitudinal study
- PMID: 28678814
- PMCID: PMC5497942
- DOI: 10.1371/journal.pmed.1002322
Long-term health status and trajectories of seriously injured patients: A population-based longitudinal study
Abstract
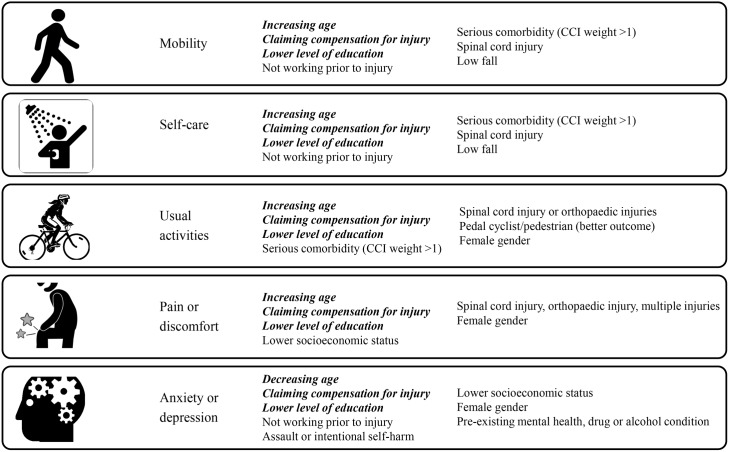
Background: Improved understanding of the quality of survival of patients is crucial in evaluating trauma care, understanding recovery patterns and timeframes, and informing healthcare, social, and disability service provision. We aimed to describe the longer-term health status of seriously injured patients, identify predictors of outcome, and establish recovery trajectories by population characteristics.
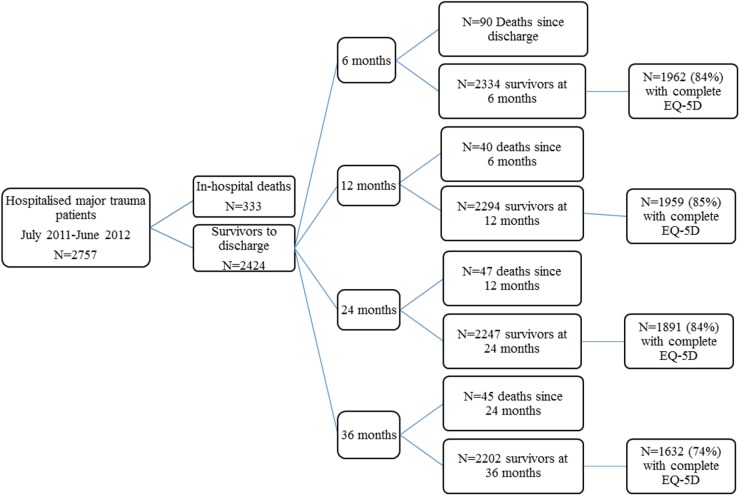
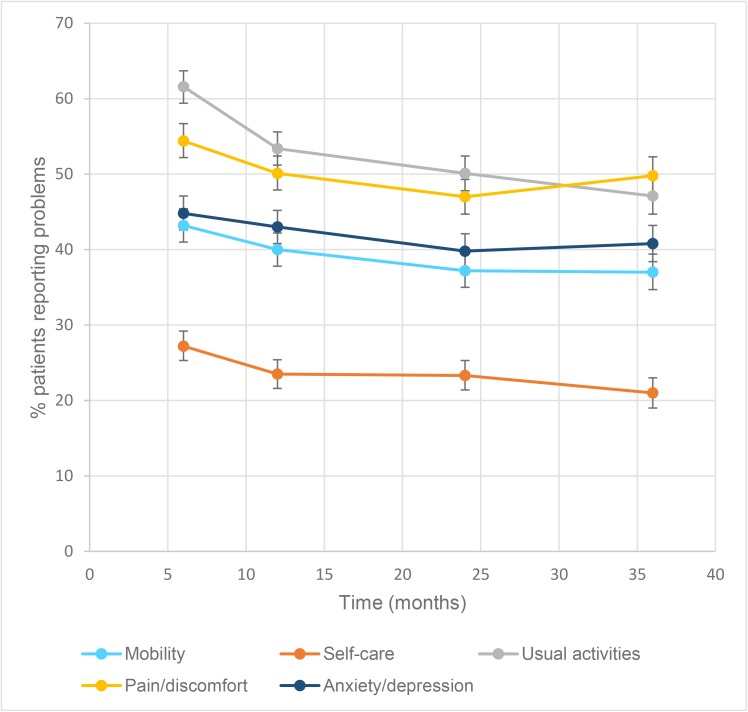
Methods and findings: A population-based, prospective cohort study using the Victorian State Trauma Registry (VSTR) was undertaken. We followed up 2,757 adult patients, injured between July 2011 and June 2012, through deaths registry linkage and telephone interview at 6-, 12-, 24-, and 36-months postinjury. The 3-level EuroQol 5 dimensions questionnaire (EQ-5D-3L) was collected, and mixed-effects regression modelling was used to identify predictors of outcome, and recovery trajectories, for the EQ-5D-3L items and summary score. Mean (SD) age of participants was 50.8 (21.6) years, and 72% were male. Twelve percent (n = 333) died during their hospital stay, 8.1% (n = 222) of patients died postdischarge, and 155 (7.0%) were known to have survived to 36-months postinjury but were lost to follow-up at all time points. The prevalence of reporting problems at 36-months postinjury was 37% for mobility, 21% for self-care, 47% for usual activities, 50% for pain/discomfort, and 41% for anxiety/depression. Continued improvement to 36-months postinjury was only present for the usual activities item; the adjusted relative risk (ARR) of reporting problems decreased from 6 to 12 (ARR 0.87, 95% CI: 0.83-0.90), 12 to 24 (ARR 0.94, 95% CI: 0.90-0.98), and 24 to 36 months (ARR 0.95, 95% CI: 0.95-0.99). The risk of reporting problems with pain or discomfort increased from 24- to 36-months postinjury (ARR 1.06, 95% CI: 1.01, 1.12). While loss to follow-up was low, there was responder bias with patients injured in intentional events, younger, and less seriously injured patients less likely to participate; therefore, these patient subgroups were underrepresented in the study findings.
Conclusions: The prevalence of ongoing problems at 3-years postinjury is high, confirming that serious injury is frequently a chronic disorder. These findings have implications for trauma system design. Investment in interventions to reduce the longer-term impact of injuries is needed, and greater investment in primary prevention is needed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Quality of life and return to work rates in the first two years following major burn injury.Burns. 2025 Apr;51(3):107355. doi: 10.1016/j.burns.2024.107355. Epub 2024 Dec 16. Burns. 2025. PMID: 39848117
-
The road to recovery for vulnerable road users hospitalised for orthopaedic injury following an on-road crash.Accid Anal Prev. 2019 Nov;132:105279. doi: 10.1016/j.aap.2019.105279. Epub 2019 Sep 3. Accid Anal Prev. 2019. PMID: 31491683
-
Cohort profile: The Trauma Outcomes Project, a prospective study of New Zealanders experiencing major trauma.BMJ Open. 2023 Nov 27;13(11):e075480. doi: 10.1136/bmjopen-2023-075480. BMJ Open. 2023. PMID: 38011969 Free PMC article.
-
Recovery after injury: an individual patient data meta-analysis of general health status using the EQ-5D.J Trauma. 2011 Oct;71(4):1003-10. doi: 10.1097/TA.0b013e3182238833. J Trauma. 2011. PMID: 21986741
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Serious Injury in Metropolitan and Regional Victoria: Exploring Travel to Treatment and Utilisation of Post-Discharge Health Services by Injury Type.Int J Environ Res Public Health. 2022 Oct 28;19(21):14063. doi: 10.3390/ijerph192114063. Int J Environ Res Public Health. 2022. PMID: 36360940 Free PMC article.
-
Epidemiology of severe trauma in Navarra for 10 years: out-of-hospital/ in-hospital deaths and survivors.BMC Emerg Med. 2023 May 24;23(1):54. doi: 10.1186/s12873-023-00818-6. BMC Emerg Med. 2023. PMID: 37226131 Free PMC article.
-
The self-assessment INTERMED predicts healthcare and social costs of orthopaedic trauma patients with persistent impairments.Clin Rehabil. 2021 Jan;35(1):135-144. doi: 10.1177/0269215520949170. Epub 2020 Aug 27. Clin Rehabil. 2021. PMID: 32851861 Free PMC article.
-
Measuring long-term outcomes after injury: current issues and future directions.Trauma Surg Acute Care Open. 2023 Mar 10;8(1):e001068. doi: 10.1136/tsaco-2022-001068. eCollection 2023. Trauma Surg Acute Care Open. 2023. PMID: 36919026 Free PMC article. Review.
-
Long-term Functional, Psychological, Emotional, and Social Outcomes in Survivors of Firearm Injuries.JAMA Surg. 2020 Jan 1;155(1):51-59. doi: 10.1001/jamasurg.2019.4533. JAMA Surg. 2020. PMID: 31746949 Free PMC article.
References
-
- Cameron P, Gabbe B, Cooper D, Walker T, Judson R, McNeil J. A statewide system of trauma care in Victoria: effect on patient survival. Med J Aust. 2008;189(10):546–50. - PubMed
-
- MacKenzie E, Rivara F, Jurkovich G, Nathens A, Egleston B, Salkever D, et al. The impact of trauma-center care on functional outcomes following major lower limb trauma. J Bone Joint Surg. 2008;90-A(1):101–9. - PubMed
-
- Nathens A, Jurkovich G, Cummings P, Rivara F, Maier R. The effect of organized systems of trauma care on motor vehicle crash mortality. J Am Med Assoc. 2000;283(15):1990–4. - PubMed
-
- Mann N, Mullins R. Research recommendations and proposed action items to facilitate trauma system implementation and evaluation. J Trauma. 1999;47(3):S75–S8. - PubMed
-
- Berwick D, Downey A, Cornett E. A National Trauma Care System to Achieve Zero Preventable Deaths After Injury—Recommendations From a National Academies of Sciences, Engineering, and Medicine Report. J Am Med Assoc. 2016;316(9):927–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
