

Pre-ESRD Depression and Post-ESRD Mortality in Patients with Advanced CKD Transitioning to Dialysis
- PMID: 28679562
- PMCID: PMC5586564
- DOI: 10.2215/CJN.00570117
Pre-ESRD Depression and Post-ESRD Mortality in Patients with Advanced CKD Transitioning to Dialysis
Abstract
Background and objectives: Depression in patients with nondialysis-dependent CKD is often undiagnosed, empirically overlooked, and associated with higher risk of death, progression to ESRD, and hospitalization. However, there is a paucity of evidence on the association between the presence of depression in patients with advanced nondialysis-dependent CKD and post-ESRD mortality, particularly among those in the transition period from late-stage nondialysis-dependent CKD to maintenance dialysis.
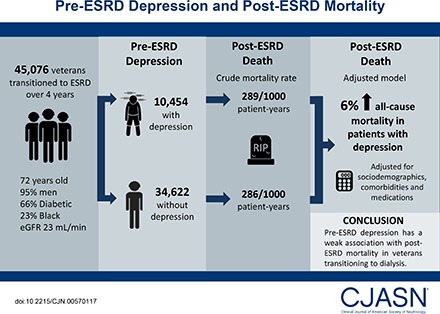
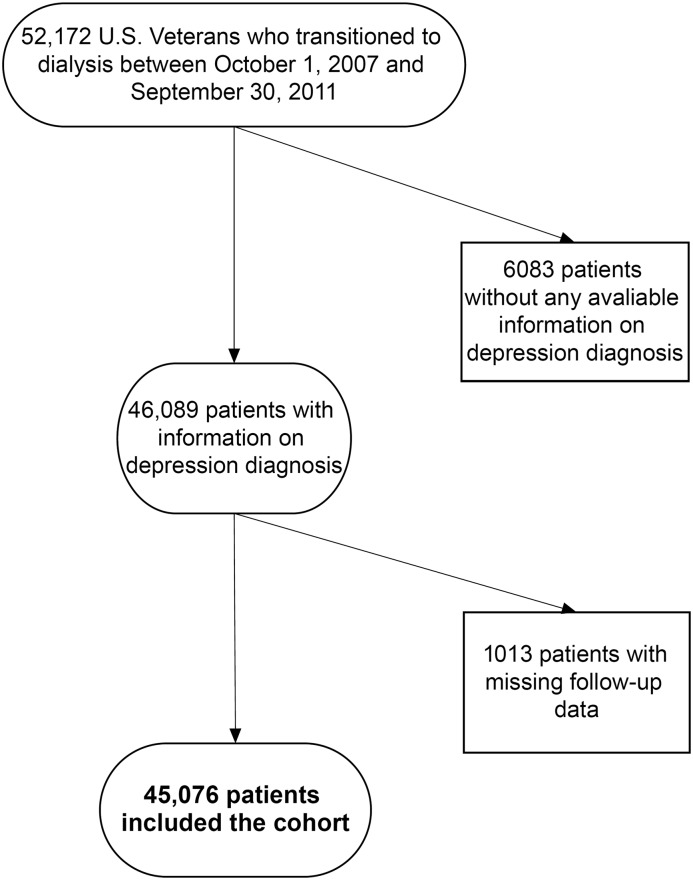
Design, setting, participants, & measurements: From a nation-wide cohort of 45,076 United States veterans who transitioned to ESRD over 4 contemporary years (November of 2007 to September of 2011), we identified 10,454 (23%) patients with a depression diagnosis during the predialysis period. We examined the association of pre-ESRD depression with all-cause mortality after transition to dialysis using Cox proportional hazards models adjusted for sociodemographics, comorbidities, and medications.
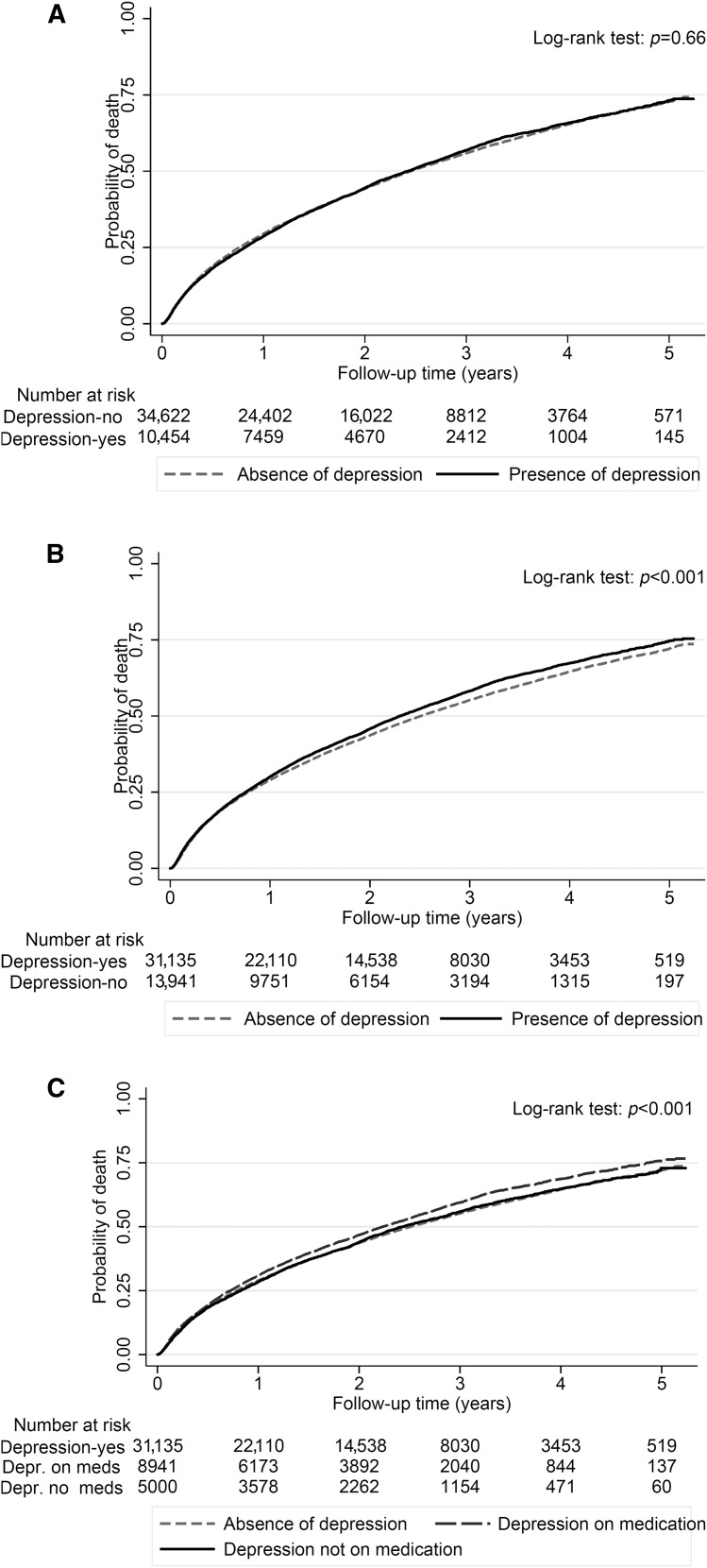
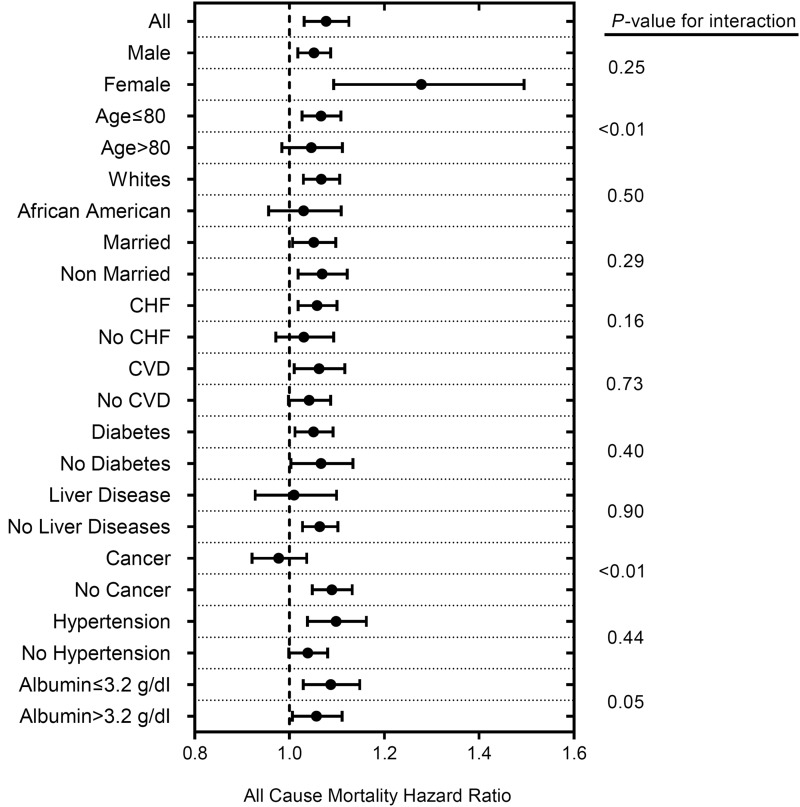
Results: Patients were 72±11 years old (mean±SD) and included 95% men, 66% patients with diabetes, and 23% blacks. The crude mortality rate was similar in patients with depression (289/1000 patient-years; 95% confidence interval, 282 to 297) versus patients without depression (286/1000 patient-years; 95% confidence interval, 282 to 290). Compared with patients without depression, patients with depression had a 6% higher all-cause mortality risk in the adjusted model (hazard ratio, 1.06; 95% confidence interval, 1.03 to 1.09). Similar results were found across all selected subgroups as well as in sensitivity analyses using alternate definitions of depression.
Conclusion: Pre-ESRD depression has a weak association with post-ESRD mortality in veterans transitioning to dialysis.
Keywords: African Americans; Comorbidity; Confidence Intervals; Disease Progression; Humans; Kidney Failure, Chronic; Male; Proportional Hazards Models; Renal Insufficiency, Chronic; Risk; Veterans; chronic kidney disease; depression; diabetes mellitus; end stage kidney disease; hospitalization; mortality; quality of life; renal dialysis; transition.
Copyright © 2017 by the American Society of Nephrology.
Figures
Similar articles
-
Association of Chronic Kidney Disease With In-Hospital Outcomes of Transcatheter Aortic Valve Replacement.JACC Cardiovasc Interv. 2017 Oct 23;10(20):2050-2060. doi: 10.1016/j.jcin.2017.07.044. JACC Cardiovasc Interv. 2017. PMID: 29050621
-
Hypoglycemia-Related Hospitalizations and Mortality Among Patients With Diabetes Transitioning to Dialysis.Am J Kidney Dis. 2018 Nov;72(5):701-710. doi: 10.1053/j.ajkd.2018.04.022. Epub 2018 Jul 20. Am J Kidney Dis. 2018. PMID: 30037725
-
The effect of increasing age on the prognosis of non-dialysis patients with chronic kidney disease receiving stable nephrology care.Kidney Int. 2012 Aug;82(4):482-8. doi: 10.1038/ki.2012.174. Kidney Int. 2012. PMID: 22622495
-
GFR at initiation of dialysis and mortality in CKD: a meta-analysis.Am J Kidney Dis. 2012 Jun;59(6):829-40. doi: 10.1053/j.ajkd.2012.01.015. Epub 2012 Apr 1. Am J Kidney Dis. 2012. PMID: 22465328 Free PMC article. Review.
-
Transition of care from pre-dialysis prelude to renal replacement therapy: the blueprints of emerging research in advanced chronic kidney disease.Nephrol Dial Transplant. 2017 Apr 1;32(suppl_2):ii91-ii98. doi: 10.1093/ndt/gfw357. Nephrol Dial Transplant. 2017. PMID: 28201698 Free PMC article. Review.
Cited by
-
Patient engagement during the transition from nondialysis-dependent chronic kidney disease to dialysis: A meta-ethnography.Health Expect. 2023 Dec;26(6):2191-2204. doi: 10.1111/hex.13850. Epub 2023 Aug 28. Health Expect. 2023. PMID: 37641530 Free PMC article.
-
Depression screening and clinical outcomes among adults initiating maintenance hemodialysis.Clin Kidney J. 2021 Jun 25;14(12):2548-2555. doi: 10.1093/ckj/sfab097. eCollection 2021 Dec. Clin Kidney J. 2021. PMID: 34950466 Free PMC article.
-
Clinical Outcomes of a Novel Multidisciplinary Care Program in Advanced Kidney Disease (PEAK).Kidney Int Rep. 2024 Jul 24;9(10):2904-2914. doi: 10.1016/j.ekir.2024.07.018. eCollection 2024 Oct. Kidney Int Rep. 2024. PMID: 39430180 Free PMC article.
-
White matter characteristics between amygdala and prefrontal cortex underlie depressive tendency in end stage renal disease patients before the dialysis initiation.Brain Imaging Behav. 2021 Aug;15(4):1815-1827. doi: 10.1007/s11682-020-00376-6. Brain Imaging Behav. 2021. PMID: 33048290
-
Depressive Symptoms Associate With Race and All-Cause Mortality in Patients With CKD.Kidney Int Rep. 2018 Oct 9;4(2):222-230. doi: 10.1016/j.ekir.2018.10.001. eCollection 2019 Feb. Kidney Int Rep. 2018. PMID: 30775619 Free PMC article.
References
-
- Cukor D, Cohen SD, Peterson RA, Kimmel PL: Psychosocial aspects of chronic disease: ESRD as a paradigmatic illness. J Am Soc Nephrol 18: 3042–3055, 2007 - PubMed
-
- Watnick S, Wang PL, Demadura T, Ganzini L: Validation of 2 depression screening tools in dialysis patients. Am J Kidney Dis 46: 919–924, 2005 - PubMed
-
- Kalender B, Ozdemir AC, Koroglu G: Association of depression with markers of nutrition and inflammation in chronic kidney disease and end-stage renal disease. Nephron Clin Pract 102: c115–c121, 2006 - PubMed
-
- Dervisoglu E, Kir HM, Kalender B, Eraldemir C, Caglayan C: Depressive symptoms and proinflammatory cytokine levels in chronic renal failure patients. Nephron Clin Pract 108: c272–c277, 2008 - PubMed
-
- Palmer S, Vecchio M, Craig JC, Tonelli M, Johnson DW, Nicolucci A, Pellegrini F, Saglimbene V, Logroscino G, Fishbane S, Strippoli GF: Prevalence of depression in chronic kidney disease: Systematic review and meta-analysis of observational studies. Kidney Int 84: 179–191, 2013 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
