

Prognostic Factor Analysis of Overall Survival in Gastric Cancer from Two Phase III Studies of Second-line Ramucirumab (REGARD and RAINBOW) Using Pooled Patient Data
- PMID: 28680718
- PMCID: PMC5489542
- DOI: 10.5230/jgc.2017.17.e16
Prognostic Factor Analysis of Overall Survival in Gastric Cancer from Two Phase III Studies of Second-line Ramucirumab (REGARD and RAINBOW) Using Pooled Patient Data
Abstract
Purpose: To identify baseline prognostic factors for survival in patients with disease progression, during or after chemotherapy for the treatment of advanced gastric or gastroesophageal junction (GEJ) cancer.
Materials and methods: We pooled data from patients randomized between 2009 and 2012 in 2 phase III, global double-blind studies of ramucirumab for the treatment of advanced gastric or GEJ adenocarcinoma following disease progression on first-line platinum- and/or fluoropyrimidine-containing therapy (REGARD and RAINBOW). Forty-one key baseline clinical and laboratory factors common in both studies were examined. Model building started with covariate screening using univariate Cox models (significance level=0.05). A stepwise multivariable Cox model identified the final prognostic factors (entry+exit significance level=0.01). Cox models were stratified by treatment and geographic region. The process was repeated to identify baseline prognostic quality of life (QoL) parameters.
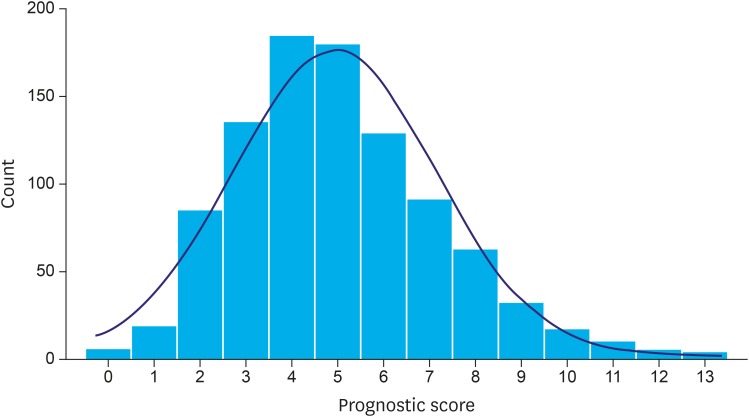
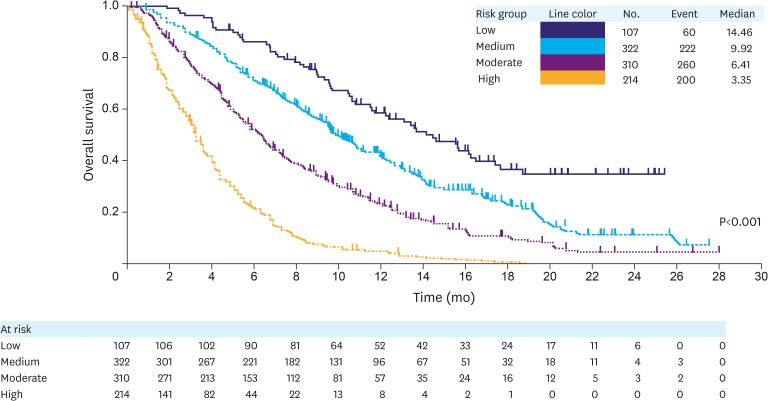
Results: Of 1,020 randomized patients, 953 (93%) patients without any missing covariates were included in the analysis. We identified 12 independent prognostic factors of poor survival: 1) peritoneal metastases; 2) Eastern Cooperative Oncology Group (ECOG) performance score 1; 3) the presence of a primary tumor; 4) time to progression since prior therapy <6 months; 5) poor/unknown tumor differentiation; abnormally low blood levels of 6) albumin, 7) sodium, and/or 8) lymphocytes; and abnormally high blood levels of 9) neutrophils, 10) aspartate aminotransferase (AST), 11) alkaline phosphatase (ALP), and/or 12) lactate dehydrogenase (LDH). Factors were used to devise a 4-tier prognostic index (median overall survival [OS] by risk [months]: high=3.4, moderate=6.4, medium=9.9, and low=14.5; Harrell's C-index=0.66; 95% confidence interval [CI], 0.64-0.68). Addition of QoL to the model identified patient-reported appetite loss as an independent prognostic factor.
Conclusions: The identified prognostic factors and the reported prognostic index may help clinical decision-making, patient stratification, and planning of future clinical studies.
Keywords: Gastroesophageal junction; Prognosis; Stomach neoplasms; Survival.
Conflict of interest statement
Conflict of Interest: Drs. Emig, Ferry, Chandrawansa, Hsu, Sashegyi, and Liepa are full-time employees and stockholders of Eli Lilly and Company. Dr. Ferry additionally received honoraria from Eli Lilly and Company, Sanofi, and Roche; he also held an advisory role for Eli Lilly and Company, Sanofi, and Roche; he received research funding from Eli Lilly and Company and Sanofi; he gave expert testimony for Eli Lilly and Company; he received travel support from Sanofi and Roche. Dr. Fuchs served as a consultant for Eli Lilly and Company, Pfizer, Entrinsic Health, Genentech, Merck, Gilead Sciences, Macrogenics, Sanofi, Dicerna, Frive Prime Therapeutics, Bristol Myers Squibb, Bayer, Merrimack, and Celgene. Dr. Muro received honoraria from Takeda, Chugai Pharma, Yakult Honsha, Merck Serono, and Taiho Pharmaceutical. Dr. Tomasek received honoraria from Roche, Bayer, Merck, Amgen, and Eli Lilly and Company; he served in an advisory role for Ipsen, Amgen, and Roche; he received research funding from Amgen, Novartis, and Eli Lilly and Company; and he received travel support from Pfizer, Eli Lily and Company, Novartis, and Roche. Dr. Van Cutsem received research support from Amgen, Bayer, Boehringer Ingelheim, Eli Lilly and Company, Merck Serono, Novartis, Roche, Sanofi, Celgene, and Ipsen. Dr. Chau would like to acknowledge United Kingdom National Health Service funding to the National Institute for Health Research Biomedical Research Centre at the Royal Marsden NHS Foundation Trust and The Institute of Cancer Research. Dr. Shimada received research funding from Eli Lilly and Company, Taiho Pharmaceutical, and Chugai Pharma. Dr. Al-Batran received honoraria and served as an advisor for Eli Lilly and Company. Dr. Passalacqua received honoraria from Eli Lilly and Company, Roche, and Novartis; he served as an advisor for Eli Lilly and Company; he is on the Speakers' bureau for Astellas Pharma; and he receives research funding from Amgen. Dr. Ohtsu is related to an employee of Celgene and he receives research funding from Bristol-Myers Squibb. Dr. Wilke received honoraria from Eli Lilly and Company and served as an advisor for Eli Lilly and Company.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet] Lyon: International Agency for Research on Cancer; [cited 2015 Aug 1]. Available from: http://globocan.iarc.fr.
-
- Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, et al., editors. SEER Cancer Statistics Review, 1975??012 (based on November 2014 SEER data submission, posted to the SEER web site, April 2015) [Internet] Bethesda (MD): National Cancer Institute; 2015. [cited 2015 Aug 1]. Available from: http://seer.cancer.gov/csr/1975_2012/
-
- Avital I, Pisters PW, Kelsen DP, Willett CG. Cancer of the stomach. In: DeVita VT, Lawrence TS, Rosenberg SA, editors. DeVita, Hellman, and Rosenberg's Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2011. pp. 924–954.
-
- Koh TJ, Wang TC. Tumors of the stomach. In: Feldman M, Friedman LS, Sleisenger MH, editors. Sleisenger & Fordtran's Gastrointestinal and Liver Disease. 7th ed. Philadelphia (PA): Saunders; 2002. pp. 829–844.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
