

Early transition to comfort measures only in acute stroke patients: Analysis from the Get With The Guidelines-Stroke registry
- PMID: 28680764
- PMCID: PMC5490382
- DOI: 10.1212/CPJ.0000000000000358
Early transition to comfort measures only in acute stroke patients: Analysis from the Get With The Guidelines-Stroke registry
Abstract
Background: Death after acute stroke often occurs after forgoing life-sustaining interventions. We sought to determine the patient and hospital characteristics associated with an early decision to transition to comfort measures only (CMO) after ischemic stroke (IS), intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH) in the Get With The Guidelines-Stroke registry.
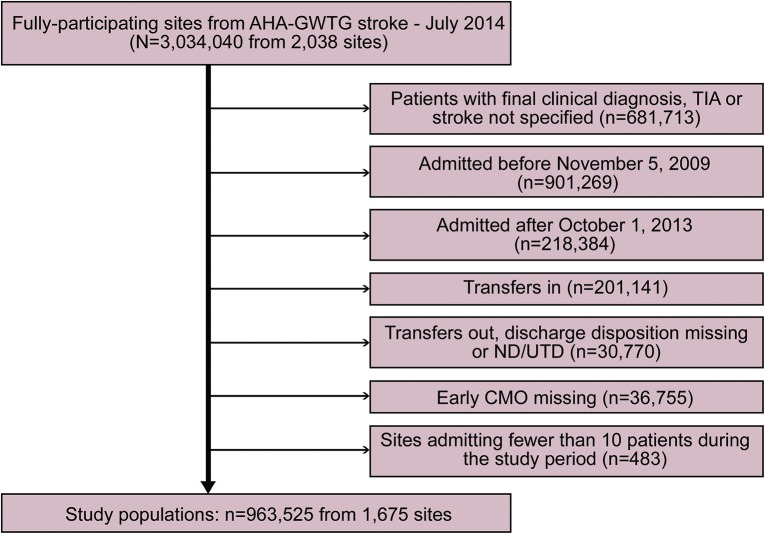
Methods: We identified patients with IS, ICH, or SAH between November 2009 and September 2013 who met study criteria. Early CMO was defined as the withdrawal of life-sustaining treatments and interventions by hospital day 0 or 1. Using multivariable logistic regression, we identified patient and hospital factors associated with an early (by hospital day 0 or 1) CMO order.
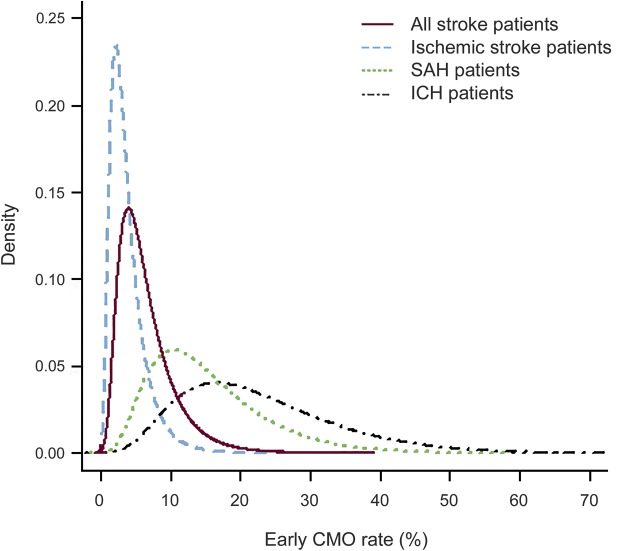
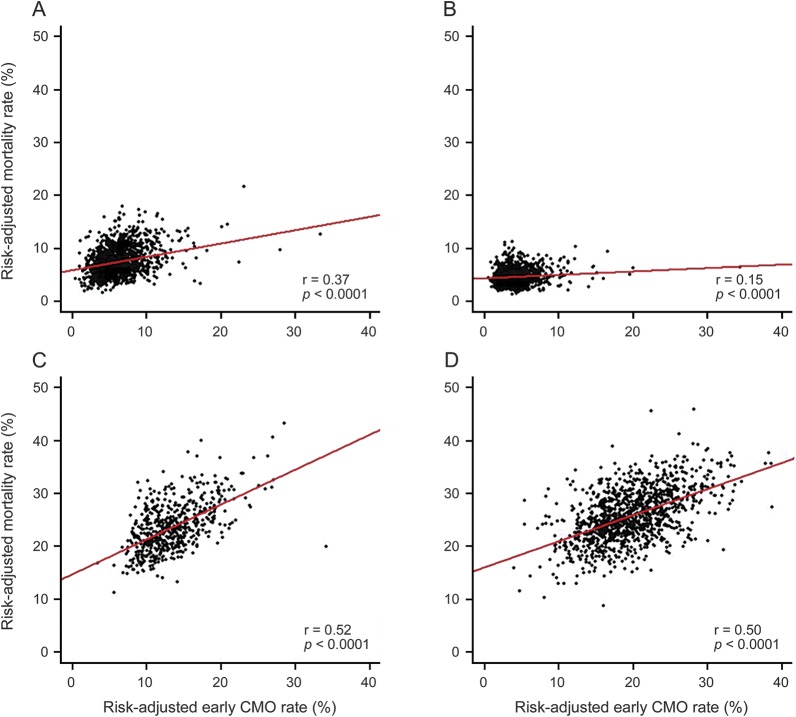
Results: Among 963,525 patients from 1,675 hospitals, 54,794 (5.6%) had an early CMO order (IS: 3.0%; ICH: 19.4%; SAH: 13.1%). Early CMO use varied widely by hospital (range 0.6%-37.6% overall) and declined over time (from 6.1% in 2009 to 5.4% in 2013; p < 0.001). In multivariable analysis, older age, female sex, white race, Medicaid and self-pay/no insurance, arrival by ambulance, arrival off-hours, baseline nonambulatory status, and stroke type were independently associated with early CMO use (vs no early CMO). The correlation between hospital-level risk-adjusted mortality and the use of early CMO was stronger for SAH (r = 0.52) and ICH (r = 0.50) than AIS (r = 0.15) patients.
Conclusions: Early CMO was utilized in about 5% of stroke patients, being more common in ICH and SAH than IS. Early CMO use varies widely between hospitals and is influenced by patient and hospital characteristics.
Figures
Comment in
-
The emerging partnership between palliative care and stroke.Neurol Clin Pract. 2017 Jun;7(3):191-193. doi: 10.1212/CPJ.0000000000000361. Neurol Clin Pract. 2017. PMID: 30107013 Free PMC article. No abstract available.
References
-
- Holloway RG, Arnold RM, Creutzfeldt CJ, et al. Palliative and end-of-life care in stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:1887–1916. - PubMed
-
- Alexandrov AV, Bladin CF, Meslin EM, Norris JW. Do-not-resuscitate orders in acute stroke. Neurology 1995;45:634–640. - PubMed
-
- Hemphill JC III, Newman J, Zhao S, Johnston SC. Hospital usage of early do-not-resuscitate orders and outcome after intracerebral hemorrhage. Stroke 2004;35:1130–1134. - PubMed
-
- Reeves MJ, Myers LJ, Williams LS, Phipps MS, Bravata DM. Do-not-resuscitate orders, quality of care, and outcomes in veterans with acute ischemic stroke. Neurology 2012;79:1990–1996. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous