

High Cellular Monocyte Activation in People Living With Human Immunodeficiency Virus on Combination Antiretroviral Therapy and Lifestyle-Matched Controls Is Associated With Greater Inflammation in Cerebrospinal Fluid
- PMID: 28680905
- PMCID: PMC5494939
- DOI: 10.1093/ofid/ofx108
High Cellular Monocyte Activation in People Living With Human Immunodeficiency Virus on Combination Antiretroviral Therapy and Lifestyle-Matched Controls Is Associated With Greater Inflammation in Cerebrospinal Fluid
Abstract
Background: Increased monocyte activation and intestinal damage have been shown to be predictive for the increased morbidity and mortality observed in treated people living with human immunodeficiency virus (PLHIV).
Methods: A cross-sectional analysis of cellular and soluble markers of monocyte activation, coagulation, intestinal damage, and inflammation in plasma and cerebrospinal fluid (CSF) of PLHIV with suppressed plasma viremia on combination antiretroviral therapy and age and demographically comparable HIV-negative individuals participating in the Comorbidity in Relation to AIDS (COBRA) cohort and, where appropriate, age-matched blood bank donors (BBD).
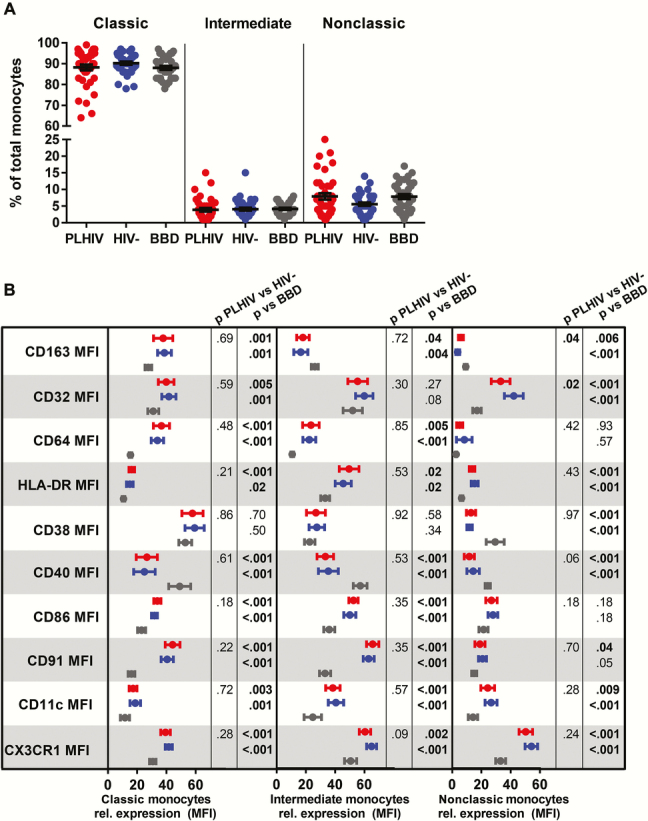
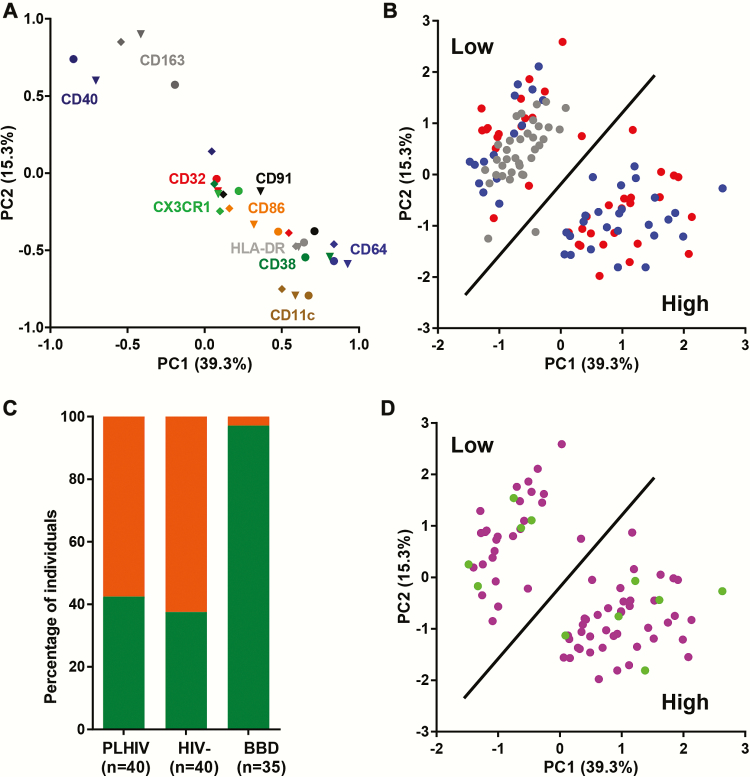
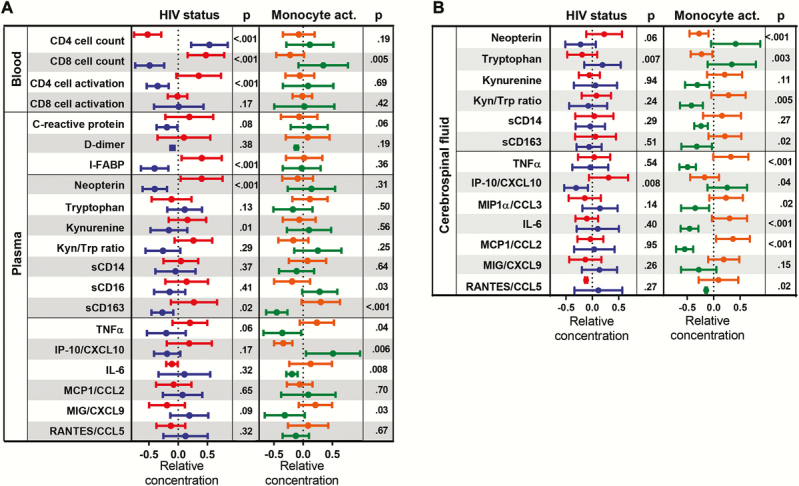
Results: People living with HIV, HIV-negative individuals, and BBD had comparable percentages of classical, intermediate, and nonclassical monocytes. Expression of CD163, CD32, CD64, HLA-DR, CD38, CD40, CD86, CD91, CD11c, and CX3CR1 on monocytes did not differ between PLHIV and HIV-negative individuals, but it differed significantly from BBD. Principal component analysis revealed that 57.5% of PLHIV and 62.5% of HIV-negative individuals had a high monocyte activation profile compared with 2.9% of BBD. Cellular monocyte activation in the COBRA cohort was strongly associated with soluble markers of monocyte activation and inflammation in the CSF.
Conclusions: People living with HIV and HIV-negative COBRA participants had high levels of cellular monocyte activation compared with age-matched BBD. High monocyte activation was predictive for inflammation in the CSF.
Keywords: CSF; HIV; immune activation; inflammation; monocyte..
© The Author 2017. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Guaraldi G, Orlando G, Zona S et al. Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin Infect Dis 2011; 53:1120–6. - PubMed
-
- Hasse B, Ledergerber B, Furrer H et al. Morbidity and aging in HIV-infected persons: the Swiss HIV cohort study. Clin Infect Dis 2011; 53:1130–9. - PubMed
-
- Schouten J, Wit FW, Stolte IG et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study. Clin Infect Dis 2014; 59:1787–97. - PubMed
-
- Brenchley JM, Price DA, Schacker TW et al. Microbial translocation is a cause of systemic immune activation in chronic HIV infection. Nat Med. 2006; 12:1365–71. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
