

Survival trends from the Prader-Willi Syndrome Association (USA) 40-year mortality survey
- PMID: 28682308
- PMCID: PMC5756527
- DOI: 10.1038/gim.2017.92
Survival trends from the Prader-Willi Syndrome Association (USA) 40-year mortality survey
Abstract
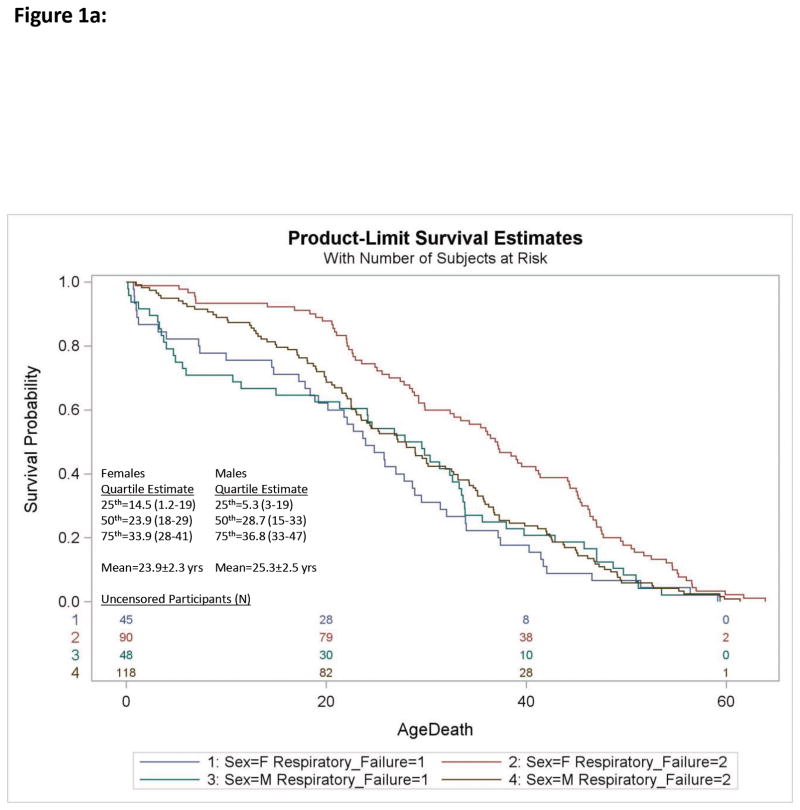
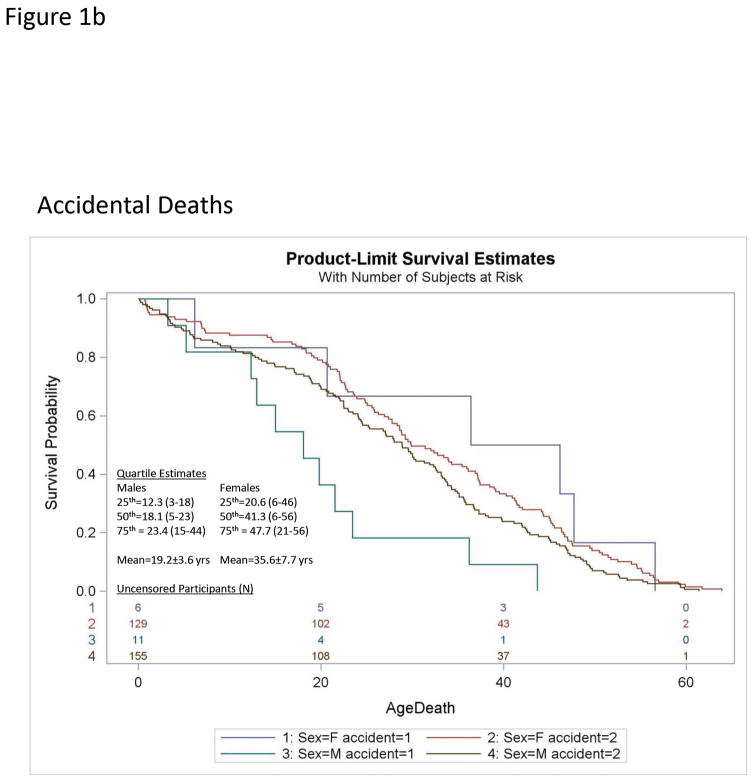
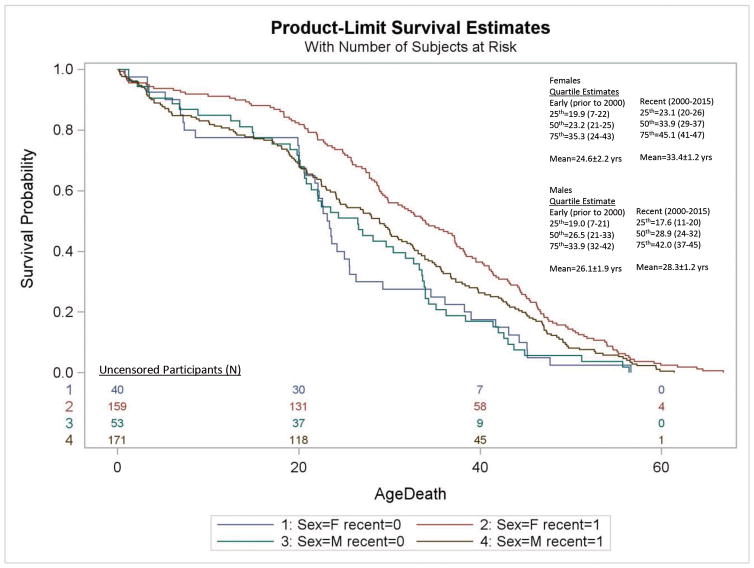
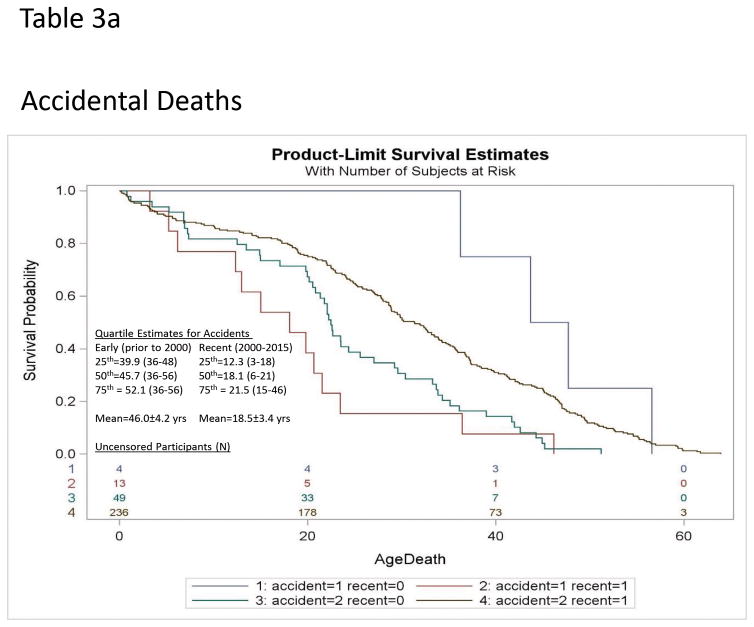
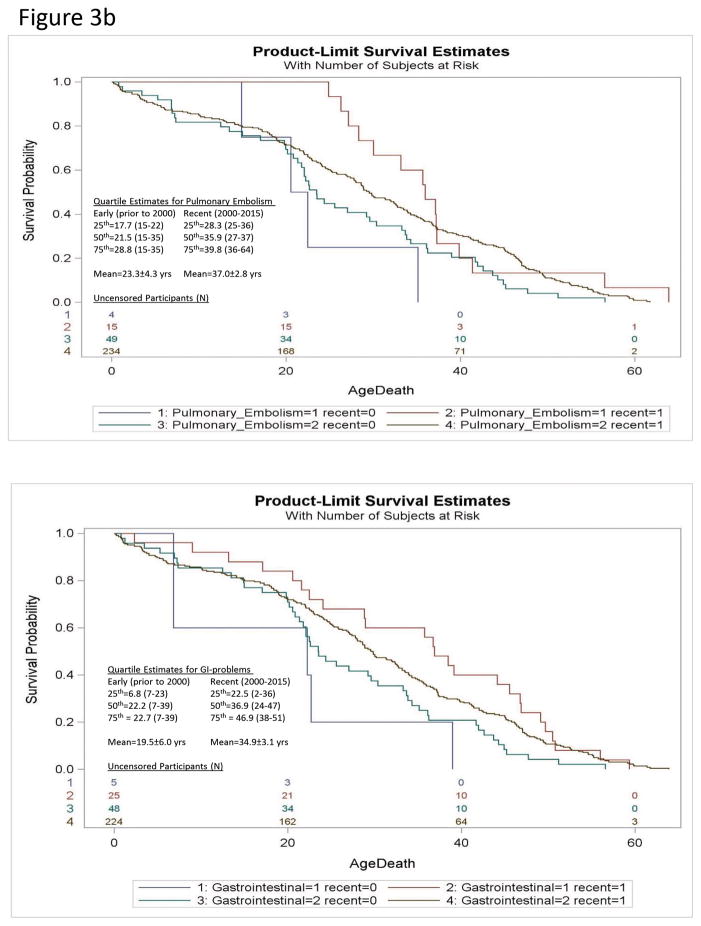
PurposePrader-Willi syndrome (PWS) is a complex genetic disorder characterized by hyperphagia and morbid obesity with increased cardiopulmonary and hyperphagia-related mortality. Survival trends in PWS were evaluated to assess the impact of modern interventions on mortality risk.MethodsThe Prader-Willi Syndrome Association (USA) 40-year mortality syndrome-specific database of 486 death reports was utilized to examine survival trends in PWS and cohort effects for recent deaths (years 2000-2015, N=331) relative to deaths prior to 2000 (N=94). Cox proportional hazards regression modeling was applied to generate log rank statistics and Kaplan-Meier curves examining sex, cause of death, and cohort.ResultsRisk for all-cause mortality in PWS was 1.5 (95% confidence interval (CI)=1.2-1.9) times higher for the Early than the Recent era cohort reflected in female cardiac failure (hazard ratio (HR)=1.8; 95% CI=1.3-2.6), pulmonary embolism (HR=6.1; 95% CI=1.7-22), and gastrointestinal-related (HR=3.2; 95% CI=1.1-7.4) causes. Accidental deaths in males increased in the Recent era cohort (HR=5.7; 95% CI=1.2-27.1), possibly due to enhanced weight management and mobility. Risk of death from respiratory failure was unchanged.ConclusionWe report measurable increases in survival effecting cardiovascular and gastrointestinal-related causes in PWS most likely attributable to earlier diagnosis and proactive interventions to prevent morbid obesity. More research is needed to address underlying vulnerability to respiratory failure, an unchanged mortality risk in PWS.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article to disclose.
The authors have no conflicts to declare.
Figures
Similar articles
-
Causes of death in Prader-Willi syndrome: Prader-Willi Syndrome Association (USA) 40-year mortality survey.Genet Med. 2017 Jun;19(6):635-642. doi: 10.1038/gim.2016.178. Epub 2016 Nov 17. Genet Med. 2017. PMID: 27854358 Free PMC article.
-
Prader-Willi syndrome in Victoria: mortality and causes of death.J Paediatr Child Health. 2012 Jun;48(6):506-11. doi: 10.1111/j.1440-1754.2011.02225.x. Epub 2011 Nov 16. J Paediatr Child Health. 2012. PMID: 22697408
-
Long-term health outcomes in patients with Prader-Willi Syndrome: a nationwide cohort study in Denmark.Int J Obes (Lond). 2017 Oct;41(10):1531-1538. doi: 10.1038/ijo.2017.139. Epub 2017 Jun 21. Int J Obes (Lond). 2017. PMID: 28634363
-
Prader-Willi syndrome and early-onset morbid obesity NIH rare disease consortium: A review of natural history study.Am J Med Genet A. 2018 Feb;176(2):368-375. doi: 10.1002/ajmg.a.38582. Epub 2017 Dec 22. Am J Med Genet A. 2018. PMID: 29271568 Free PMC article. Review.
-
Review of 64 cases of death in children with Prader-Willi syndrome (PWS).Am J Med Genet A. 2008 Apr 1;146A(7):881-7. doi: 10.1002/ajmg.a.32131. Am J Med Genet A. 2008. PMID: 18324685 Review.
Cited by
-
Successful peritoneal dialysis for the end-stage kidney disease associated with Prader-Willi syndrome: a case report.CEN Case Rep. 2019 Aug;8(3):216-220. doi: 10.1007/s13730-019-00395-3. Epub 2019 Apr 8. CEN Case Rep. 2019. PMID: 30963414 Free PMC article.
-
Caring and living with Prader-Willi syndrome in Italy: integrating children, adults and parents' experiences through a multicentre narrative medicine research.BMJ Open. 2020 Aug 6;10(8):e036502. doi: 10.1136/bmjopen-2019-036502. BMJ Open. 2020. PMID: 32764084 Free PMC article.
-
Genetic conditions of short stature: A review of three classic examples.Front Endocrinol (Lausanne). 2022 Oct 21;13:1011960. doi: 10.3389/fendo.2022.1011960. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36339399 Free PMC article. Review.
-
Venous Thromboembolism in Prader-Willi Syndrome: A Questionnaire Survey.Genes (Basel). 2019 Jul 19;10(7):550. doi: 10.3390/genes10070550. Genes (Basel). 2019. PMID: 31331040 Free PMC article.
-
Thrombosis Risk History and D-dimer Levels in Asymptomatic Individuals with Prader-Willi Syndrome.J Clin Med. 2022 Apr 5;11(7):2040. doi: 10.3390/jcm11072040. J Clin Med. 2022. PMID: 35407648 Free PMC article.
References
-
- Butler MG, Lee PDK, Whitman BY, editors. Management of Prader-Willi Syndrome. 3. New York: Springer; 2006.
-
- Cassidy SB, Schwartz S, Miller JL, Driscoll DJ. Prader-Willi syndrome. Genet Med. 2012;14(1):10–26. - PubMed
-
- Hoybye C, editor. Laboratory and Clinical Research. New York: Nova Science Publishers, Inc; 2013. Prader-Will Syndrome. Congenital Disorders.
-
- Butler JV, Whittington JE, Holland AJ, Boer H, Clarke D, Webb T. Prevalence of, and risk factors for, physical ill-health in people with Prader-Willi syndrome. a population-based study. Dev Med Child Neurol. 2002;44(4):248–255. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
