

Accommodation and related conditions in vascularized composite allografts
- PMID: 28682798
- PMCID: PMC5648361
- DOI: 10.1097/MOT.0000000000000446
Accommodation and related conditions in vascularized composite allografts
Abstract
Purpose of review: The outcome of vascularized composite allografts (VCA) often appear unrelated to the presence of donor-specific antibodies (DSA) in blood of the recipient or deposition of complement in the graft. The attenuation of injury and the absence of rejection in other types of grafts despite manifest donor-specific immunity have been explained by accommodation (acquired resistance to immune-mediated injury), adaptation (loss of graft antigen) and/or enhancement (antibody-mediated antigen blockade). Whether and how accommodation, adaptation and/or enhancement impact on the outcome of VCA is unknown. Here we consider how recent observations concerning accommodation in organ transplants might advance understanding and resolve uncertainties about the clinical course of VCA.
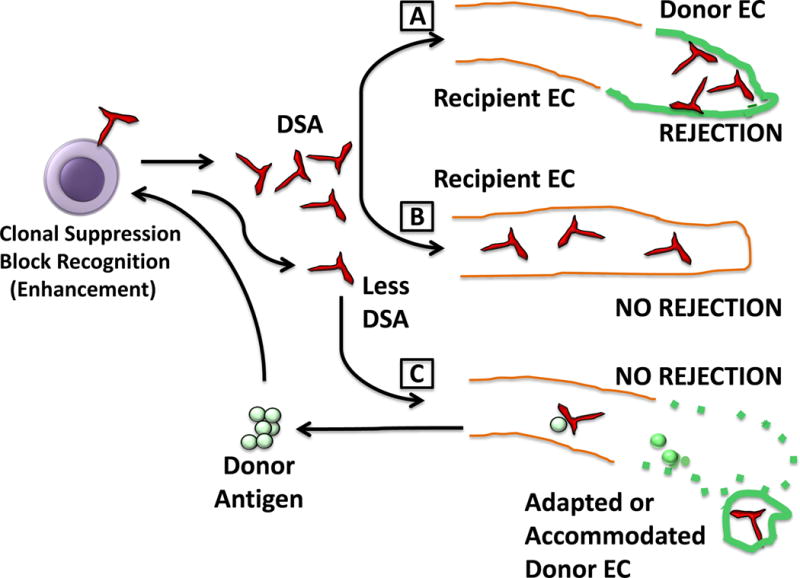
Recent findings: Investigation of the mechanisms through which kidney allografts avert antibody-mediated injury and rejection provide insights potentially applicable to VCA. Interaction of DSA can facilitate replacement of donor by recipient endothelial cells, modulate or decrease synthesis of antigen, mobilize antigen that in turn blocks further immune recognition and limit the amount of bound antibody, allowing accommodation to ensue. These processes also can explain the apparent dissociation between the presence and levels of DSA in blood, deposition of C4d in grafts and antibody-mediated rejection. Over time the processes might also explain the inception of chronic graft changes.
Summary: The disrupted tissue in VCA and potential for repopulation by endothelial cells of the recipient establish conditions that potentially decrease susceptibility to acute antibody-mediated rejection. These conditions include clonal suppression of donor-specific B cells, and adaptation, enhancement and accommodation. This setting also potentially highlights heretofore unrecognized interactions between these 'protective' processes.
Conflict of interest statement
none
Figures
Similar articles
-
Graft vasculopathy of vascularized composite allografts in humans: a literature review and retrospective study.Transpl Int. 2019 Aug;32(8):831-838. doi: 10.1111/tri.13421. Epub 2019 Apr 2. Transpl Int. 2019. PMID: 30829423 Review.
-
Chronic rejection in vascularized composite allografts.Curr Opin Organ Transplant. 2014 Jun;19(3):309-14. doi: 10.1097/MOT.0000000000000073. Curr Opin Organ Transplant. 2014. PMID: 24811439 Review.
-
Donor-specific antibodies and antibody-mediated rejection in vascularized composite allotransplantation.Curr Opin Organ Transplant. 2016 Oct;21(5):510-5. doi: 10.1097/MOT.0000000000000349. Curr Opin Organ Transplant. 2016. PMID: 27517505 Review.
-
Immunological and inflammatory mapping of vascularized composite allograft rejection processes in a rat model.PLoS One. 2017 Jul 26;12(7):e0181507. doi: 10.1371/journal.pone.0181507. eCollection 2017. PLoS One. 2017. PMID: 28746417 Free PMC article.
-
Immunopathology of rejection: do the rules of solid organ apply to vascularized composite allotransplantation?Curr Opin Organ Transplant. 2015 Dec;20(6):596-601. doi: 10.1097/MOT.0000000000000242. Curr Opin Organ Transplant. 2015. PMID: 26536419 Review.
Cited by
-
Non-canonical B cell functions in transplantation.Hum Immunol. 2019 Jun;80(6):363-377. doi: 10.1016/j.humimm.2019.04.006. Epub 2019 Apr 10. Hum Immunol. 2019. PMID: 30980861 Free PMC article. Review.
-
TNFRSF13B in B cell responses to organ transplantation.Hum Immunol. 2023 Jan;84(1):27-33. doi: 10.1016/j.humimm.2022.09.006. Epub 2022 Nov 1. Hum Immunol. 2023. PMID: 36333165 Free PMC article.
-
Cellular activation pathways and interaction networks in vascularized composite allotransplantation.Front Immunol. 2023 May 17;14:1179355. doi: 10.3389/fimmu.2023.1179355. eCollection 2023. Front Immunol. 2023. PMID: 37266446 Free PMC article. Review.
-
Toward a solution for cardiac failure in the newborn.Xenotransplantation. 2018 Nov;25(6):e12479. doi: 10.1111/xen.12479. Epub 2018 Dec 11. Xenotransplantation. 2018. PMID: 30537350 Free PMC article. Review.
-
Clinical and preclinical tolerance protocols for vascularized composite allograft transplantation.Arch Plast Surg. 2021 Nov;48(6):703-713. doi: 10.5999/aps.2021.00927. Epub 2021 Nov 15. Arch Plast Surg. 2021. PMID: 34818720 Free PMC article.
References
-
- Koch CA, Khalpey ZI, Platt JL. Accommodation: preventing injury in transplantation and disease. J Immunol. 2004;172:5143–8. - PubMed
-
- Chopek MW, Simmons RL, Platt JL. ABO-incompatible renal transplantation: initial immunopathologic evaluation. Transplantation Proceedings. 1987;19:4553–7. - PubMed
-
- Platt JL, Vercellotti GM, Dalmasso AP, Matas AJ, Bolman RM, Najarian JS, et al. Transplantation of discordant xenografts: a review of progress. Immunology Today. 1990;11:450–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
