

Gait deficiencies associated with peripheral artery disease are different than chronic obstructive pulmonary disease
- PMID: 28683417
- PMCID: PMC5563974
- DOI: 10.1016/j.gaitpost.2017.06.018
Gait deficiencies associated with peripheral artery disease are different than chronic obstructive pulmonary disease
Abstract
Objective: Previous studies have indicated that patients with peripheral artery disease (PAD), display significant differences in their kinetic and kinematic gait characteristics when compared to healthy, aged-matched controls. The ability of patients with chronic obstructive pulmonary disease (COPD) to ambulate is also limited. These limitations are likely due to pathology-driven muscle morphology and physiology alterations establish in PAD and COP, respectively. Gait changes in PAD were compared to gait changes due to COPD to further understand how altered limb muscle due to disease can alter walking patterns. Both groups were independently compared to healthy controls. It was hypothesized that both patients with PAD and COPD would demonstrate similar differences in gait when compared to healthy controls.
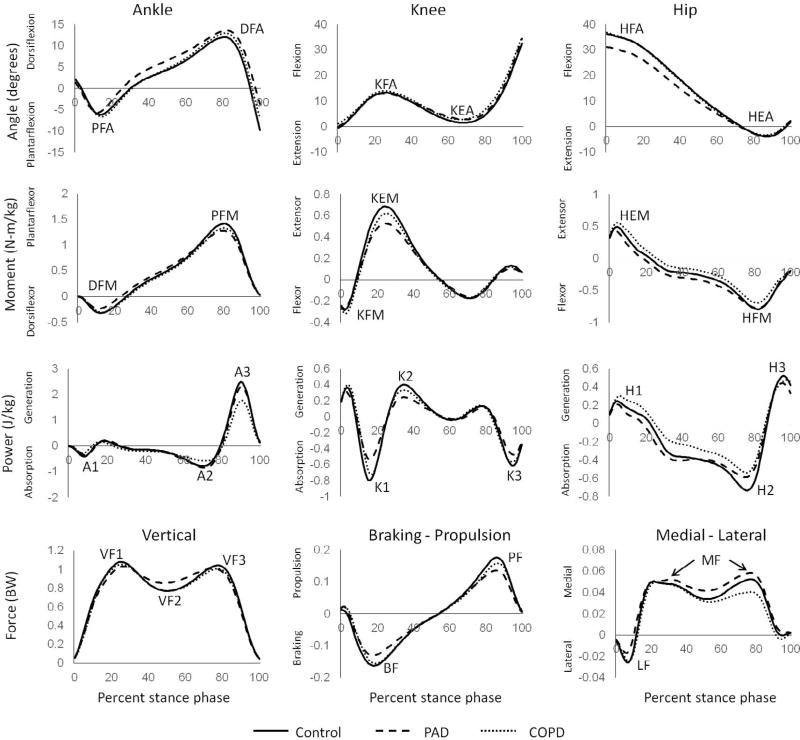
Methods: Patients with PAD (n=25), patients with COPD (n=16), and healthy older control subjects (n=25) performed five walking trials at self-selected speeds. Sagittal plane joint kinematic and kinetic group means were compared.
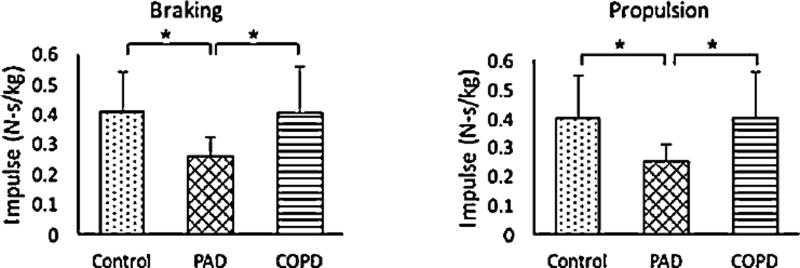
Results: Peak values for hip flexion angle, braking impulse, and propulsive impulse were significantly reduced in patients with symptomatic PAD compared to patients with COPD. After adjusting for walking velocity, significant reductions (p<0.05) in the peak values for hip flexion angle, dorsiflexor moment, ankle power generation, propulsion force, braking impulse, and propulsive impulse were found in patients with PAD compared to healthy controls. No significant differences were observed between patients with COPD and controls.
Conclusions: The results of this study demonstrate that while gait patterns are impaired for patients with PAD, this is not apparent for patients with COPD (without PAD). PAD (without COPD) causes changes to the muscle function of the lower limbs that affects gait even when subjects walk from a fully rested state. Altered muscle function in patients with COPD does not have a similar effect.
Keywords: Chronic obstructive pulmonary disease; Gait; Kinematics; Kinetics; Peripheral artery disease; Vascular disease.
Copyright © 2017 Elsevier B.V. All rights reserved.
Conflict of interest statement
Eric Pisciotta, John McCamley, Shane Wurdeman, Iraklis Pipinos, Jason Johanning, Sara Myers, and Jenna Yentes, declare no conflicts of interest.
Figures
Similar articles
-
Gait kinematics and kinetics are affected more by peripheral arterial disease than by age.J Rehabil Res Dev. 2016;53(2):229-38. doi: 10.1682/JRRD.2015.02.0027. J Rehabil Res Dev. 2016. PMID: 27149635 Free PMC article.
-
Peripheral arterial disease affects kinematics during walking.J Vasc Surg. 2009 Jan;49(1):127-32. doi: 10.1016/j.jvs.2008.08.013. Epub 2008 Nov 22. J Vasc Surg. 2009. PMID: 19028062
-
Joint torques and powers are reduced during ambulation for both limbs in patients with unilateral claudication.J Vasc Surg. 2010 Jan;51(1):80-8. doi: 10.1016/j.jvs.2009.07.117. Epub 2009 Oct 17. J Vasc Surg. 2010. PMID: 19837536 Free PMC article.
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
The Comorbidity of Chronic Obstructive Pulmonary Disease and Peripheral Artery Disease - A Systematic Review.COPD. 2019 Aug;16(3-4):292-302. doi: 10.1080/15412555.2019.1653271. Epub 2019 Sep 5. COPD. 2019. PMID: 31581921
Cited by
-
Lower limb revascularization leads to faster walking but with less efficient mechanics in claudicating patients.J Biomech. 2024 Jan;162:111880. doi: 10.1016/j.jbiomech.2023.111880. Epub 2023 Nov 22. J Biomech. 2024. PMID: 38070293 Free PMC article.
-
A Preliminary Study on Kinetic Analysis of Ground Reaction Force and Impulse During Gait in Patients With Total Hip Replacement and Implication for Rehabilitation.Orthop Surg. 2024 Dec;16(12):3162-3178. doi: 10.1111/os.14276. Epub 2024 Oct 30. Orthop Surg. 2024. PMID: 39475002 Free PMC article.
-
A biomechanical perspective on walking in patients with peripheral artery disease.Vasc Med. 2023 Feb;28(1):77-84. doi: 10.1177/1358863X221146207. Vasc Med. 2023. PMID: 36759931 Free PMC article. Review.
-
Technologies for the Instrumental Evaluation of Physical Function in Persons Affected by Chronic Obstructive Pulmonary Disease: A Systematic Review.Sensors (Basel). 2022 Sep 1;22(17):6620. doi: 10.3390/s22176620. Sensors (Basel). 2022. PMID: 36081078 Free PMC article.
-
Patient perspectives of ankle-foot orthoses for walking ability in peripheral artery disease: A qualitative study.J Vasc Nurs. 2020 Sep;38(3):100-107. doi: 10.1016/j.jvn.2020.07.004. Epub 2020 Aug 10. J Vasc Nurs. 2020. PMID: 32950110 Free PMC article.
References
-
- Brass EP, Hiatt WR, Green S. Skeletal muscle metabolic changes in peripheral arterial disease contribute to exercise intolerance: a point-counterpoint discussion. Vasc. Med. 2004;9:293–301. http://dx.doi.org/10.1191/1358863x04vm572ra. - DOI - PubMed
-
- Saey D, Côté CH, Mador MJ, Laviolette L, Leblanc P, Jobin J, et al. Assessment of muscle fatigue during exercise in chronic obstructive pulmonary disease. Muscle Nerve. 2006;34:62–71. http://dx.doi.org/10.1002/mus.20541. - DOI - PubMed
-
- McDermott MM, Hoff F, Ferrucci L, Pearce WH, Guralnik JM, Tian L, et al. Lower extremity ischemia, calf skeletal muscle characteristics, and functional impairment in peripheral arterial disease. J. Am. Geriatr. Soc. 2007;55:400–406. http://dx.doi.org/10.1111/j.1532-5415.2007.01092.x. - DOI - PMC - PubMed
-
- Gagnon P, Maltais F, Bouyer L, Ribeiro F, Coats V, Brouillard C, et al. Distal leg muscle function in patients with COPD. COPD. 2013;10:235–242. http://dx.doi.org/10.3109/15412555.2012.719047. - DOI - PubMed
-
- Roig M, Eng JJ, MacIntyre DL, Road JD, Reid WD. Deficits in muscle strength, mass quality, and mobility in people with chronic obstructive pulmonary disease. J. Cardiopulm. Rehabil. Prev. 2011;31:120–124. http://dx.doi.org/10.1097/HCR.0b013e3181f68ae4. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
