

Multifocal pigmented villonodular synovitis coexisting in both the knee joint and the patella: a case report and literature review
- PMID: 28683727
- PMCID: PMC5501528
- DOI: 10.1186/s12891-017-1654-6
Multifocal pigmented villonodular synovitis coexisting in both the knee joint and the patella: a case report and literature review
Abstract
Backgroud: Pigmented villonodular synovitis (PVNS) is an uncommon entity of proliferative lesion of the synovium, presenting with different clinical signs and symptoms. PVNS rarely forms an osteolytic lesion in a bone. Here we report a unique case of PVNS with a nodular lesion in the left patella.
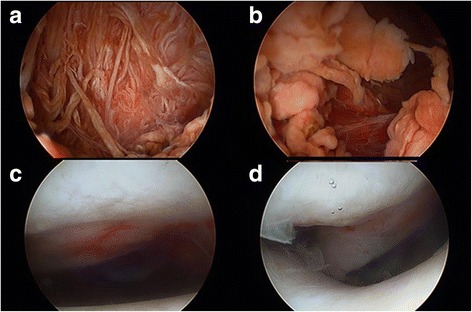
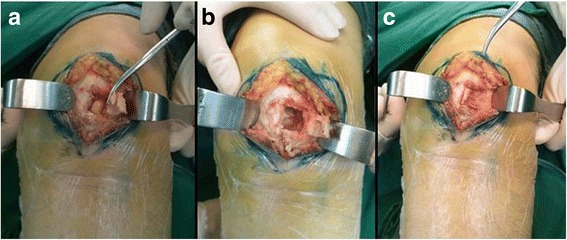
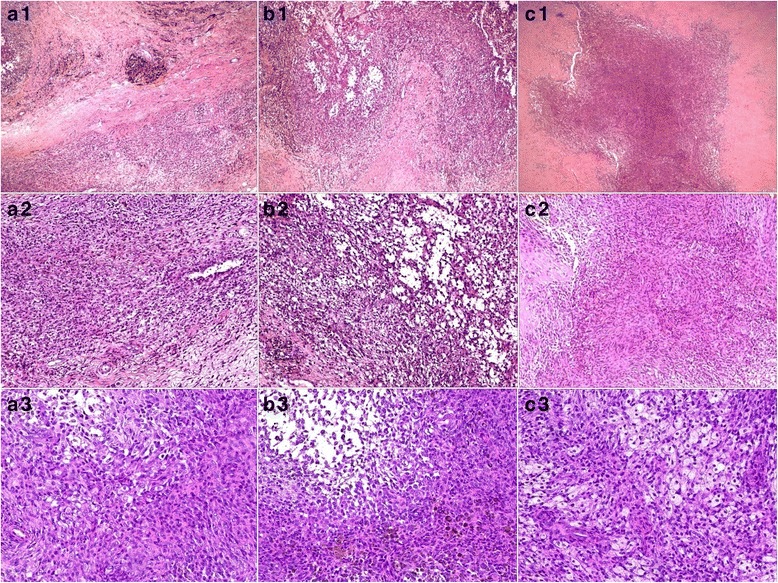
Case presentation: A 37-year-old female was referred to our hospital with complaints of ongoing left knee pain and a painful and palpable mass in her left popliteal fossa. MRI demonstrated a nodular lesion in the left patella, diffuse affected synovial tissue in the left knee and an extra-articular mass in the left popliteal fossa. After a primary diagnosis of PVNS had been established, combined arthroscopic synovectomy and open resection were performed. The postoperative pathological diagnoses of the resected mass from the popliteal fossa, the affected synovial tissue and the lesion in the patella were consistent with PVNS. At 1-year follow-up, no evidence of recurrence was noted.
Conclusions: Based on brief literature review of PNVS, we presented a very rare case of PVNS with a nodular lesion in the left patella, diffuse affected synovial tissue in the left knee and an extra-articular mass in the left popliteal fossa.
Keywords: Case report; Giant cell tumor of tendon sheath; Localized form; Multifocal lesions; Patella; Pigmented villonodular synovitis; Popliteal fossa.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Executive Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
