

Intravenous neutralization of vascular endothelial growth factor reduces vascular function/permeability of the ovary and prevents development of OHSS-like symptoms in rhesus monkeys
- PMID: 28683759
- PMCID: PMC5501270
- DOI: 10.1186/s13048-017-0340-5
Intravenous neutralization of vascular endothelial growth factor reduces vascular function/permeability of the ovary and prevents development of OHSS-like symptoms in rhesus monkeys
Abstract
Background: Ovarian hyperstimulation syndrome (OHSS) is a disorder associated with elevated serum VEGFA following chorionic gonadotropin (hCG) exposure in controlled ovarian stimulation (COS) cycles in women. In this study, we tested the effect of intravenous VEGFA neutralization on OHSS-like symptoms and vascular function in rhesus macaques during COS cycles.
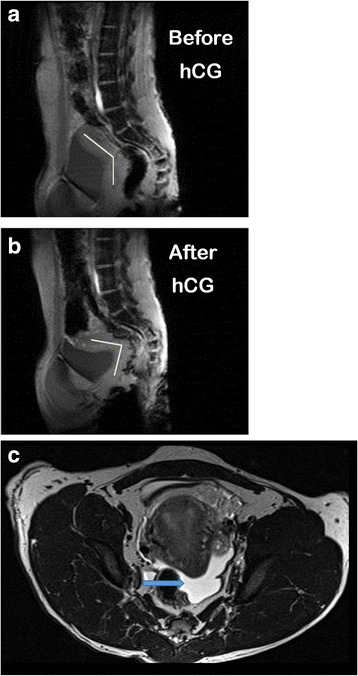
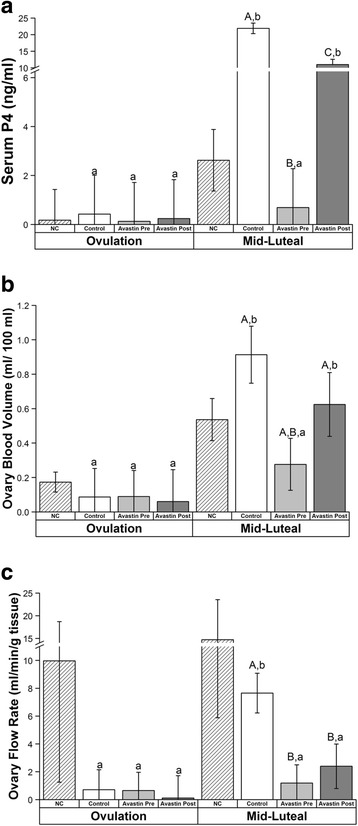
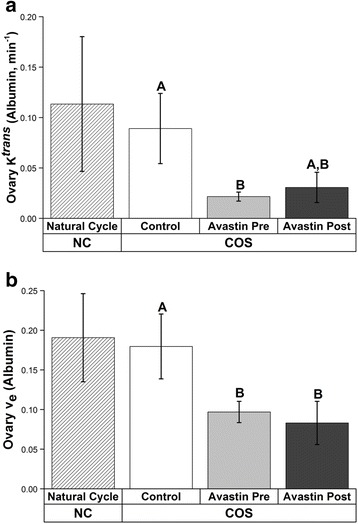
Methods: Monkeys (n = 8) were treated with 3 COS protocols and assigned randomly to groups as follows: 1) COS alone (Control, n = 5); 2) COS + VEGF mAb Avastin 19 ± 5 h before hCG (Avastin pre-hCG; n = 6); 3) COS + Avastin 3-4 days post-hCG (Avastin post-hCG; n = 4); 4) COS + Simulated Early Pregnancy (SEP n = 3); or 5) COS + SEP + Avastin (SEP + Avastin n = 3). Follicles were aspirated 36 h post-hCG, fluid was collected from one follicle for analysis of steroid and vascular hormone content. Remaining follicles were aspirated, and luteinized granulosa cells (LGCs) cultured for 24 h. Ovarian/uterine vascular flow (VF) and blood volume (BV) were analyzed by contrast enhanced ultrasound (CEUS) before hCG bolus and 6-8 days post-hCG bolus/time of peak SEP response. Ovarian permeability to albumin was analyzed by Dynamic Contrast Enhanced-MRI (DCE-MRI) post-hCG.
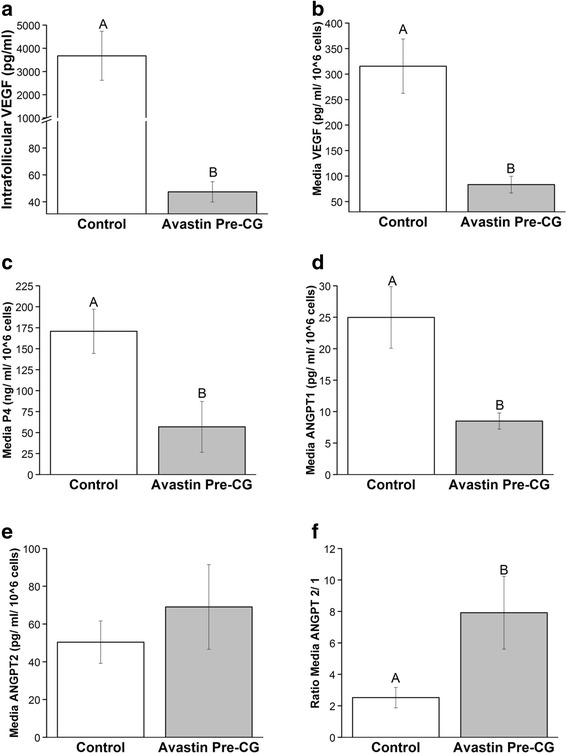
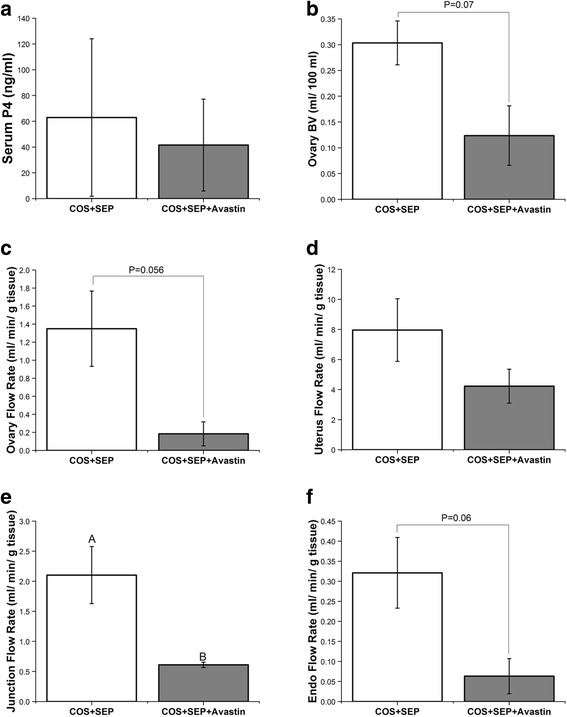
Results: Abdominal fluid was present in 4/5 Control, 2/6 Avastin pre-hCG, and 3/4 Avastin post-hCG females. Neutralization of VEGFA before hCG reduced ovarian VF, BV, and permeability to albumin (P < 0.05), while only ovarian VF and permeability were reduced in Avastin-post hCG group (P < 0.05). There was no effect of Avastin on ovarian vascular function during COS + SEP. VEGF levels in follicular fluid were reduced 78-fold by Avastin pre-hCG, and LGCs exposed to Avastin in vivo also released 4-fold less VEGF into culture media (P < 0.05). Culture medium of LGCs exposed to VEGFA neutralization in vivo had lower levels of P4 and ANGPT1, and an increased ratio of ANGPT2/1 (P < 0.05). Uterine VF was reduced by SEP + Avastin in the basalis/junctional zone (P < 0.05).
Conclusions: Avastin treatment before hCG prevents the development of symptoms associated with ovarian hyperstimulation syndrome. In vitro data suggest neutralization of VEGFA alters expression of other vascular factors typically induced by hCG in the luteinizing follicle. Neutralization of VEGFA action alters the vascular function of the basalis zone of the uterus during simulated early pregnancy, indicating a potential effect on embryo implantation.
Keywords: Chorionic Gonadotropin; Controlled ovarian stimulation; Ovarian vascular function; Uterine vascular function; VEGFA.
Conflict of interest statement
Ethics approval
All procedures and protocols were approved by the Oregon Health & Science University (OHSU)/Oregon National Primate Research Center (ONPRC) institutional animal care and use committee (IACUC) in accordance with the U.S. Public Health Service (PHS) Policy on Humane Care and Use of Laboratory Animals.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Prevention of the onset of ovarian hyperstimulation syndrome (OHSS) in the rat after ovulation induction with a low molecular weight agonist of the LH receptor compared with hCG and rec-LH.Endocrinology. 2011 Nov;152(11):4350-7. doi: 10.1210/en.2011-1077. Epub 2011 Sep 6. Endocrinology. 2011. PMID: 21896671
-
Human chorionic gonadotropin-induced ovarian hyperstimulation syndrome is associated with up-regulation of vascular endothelial growth factor.J Clin Endocrinol Metab. 2002 Jul;87(7):3300-8. doi: 10.1210/jcem.87.7.8651. J Clin Endocrinol Metab. 2002. PMID: 12107240
-
Molecular mechanisms of ovarian hyperstimulation syndrome: paracrine reduction of endothelial claudin 5 by hCG in vitro is associated with increased endothelial permeability.Hum Reprod. 2009 May;24(5):1191-9. doi: 10.1093/humrep/den479. Epub 2009 Jan 24. Hum Reprod. 2009. PMID: 19168871
-
The role of vascular endothelial growth factor and interleukins in the pathogenesis of severe ovarian hyperstimulation syndrome.Hum Reprod Update. 1997 May-Jun;3(3):255-66. doi: 10.1093/humupd/3.3.255. Hum Reprod Update. 1997. PMID: 9322101 Review.
-
Targeting the vascular endothelial growth factor system to prevent ovarian hyperstimulation syndrome.Hum Reprod Update. 2008 Jul-Aug;14(4):321-33. doi: 10.1093/humupd/dmn008. Epub 2008 Apr 2. Hum Reprod Update. 2008. PMID: 18385260 Review.
Cited by
-
TGF-β1 induces VEGF expression in human granulosa-lutein cells: a potential mechanism for the pathogenesis of ovarian hyperstimulation syndrome.Exp Mol Med. 2020 Mar;52(3):450-460. doi: 10.1038/s12276-020-0396-y. Epub 2020 Mar 10. Exp Mol Med. 2020. PMID: 32152452 Free PMC article.
-
Contrast-Enhanced Ultrasonography (CEUS) in Imaging of the Reproductive System in Dogs: A Literature Review.Animals (Basel). 2023 May 11;13(10):1615. doi: 10.3390/ani13101615. Animals (Basel). 2023. PMID: 37238045 Free PMC article. Review.
-
Chronic hyperandrogenemia in the presence and absence of a western-style diet impairs ovarian and uterine structure/function in young adult rhesus monkeys.Hum Reprod. 2018 Jan 1;33(1):128-139. doi: 10.1093/humrep/dex338. Hum Reprod. 2018. PMID: 29190387 Free PMC article.
-
The Therapeutic Potential of EGCG and Pro-EGCG in Mitigating Ovarian Hyperstimulation Syndrome: Unraveling the Modulatory Mechanism through the VEGF Pathway.Int J Biol Sci. 2025 Apr 22;21(7):3045-3060. doi: 10.7150/ijbs.98653. eCollection 2025. Int J Biol Sci. 2025. PMID: 40384868 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
