

User-fee-removal improves equity of children's health care utilization and reduces families' financial burden: evidence from Jamaica
- PMID: 28685038
- PMCID: PMC5481893
- DOI: 10.7189/jogh.07.010502
User-fee-removal improves equity of children's health care utilization and reduces families' financial burden: evidence from Jamaica
Abstract
Background: The impact of user-fee policies on the equity of health care utilization and households' financial burdens has remained largely unexplored in Latin American and the Caribbean, as well as in upper-middle-income countries. This paper assesses the short- and long-term impacts of Jamaica's user-fee-removal for children in 2007.
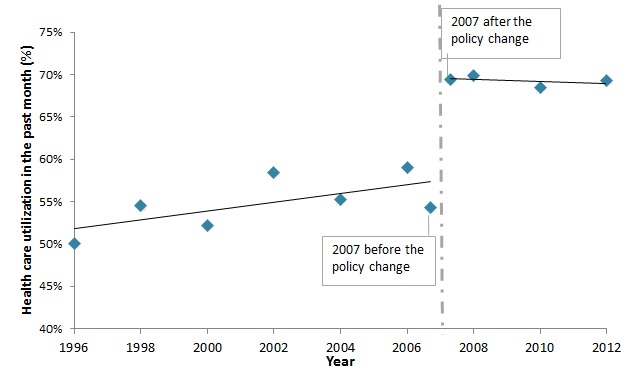
Methods: This study utilizes 14 rounds of data from the Jamaica Survey of Living Conditions (JSLC) for the periods 1996 to 2012. JSLC is a national household survey, which collects data on health care utilization and among other purposes for planning. Interrupted time series (ITS) analysis was used to examine the immediate impact of the user-fee-removal policy on children's health care utilization and households' financial burdens, as well as the impact in the medium- to long-term.
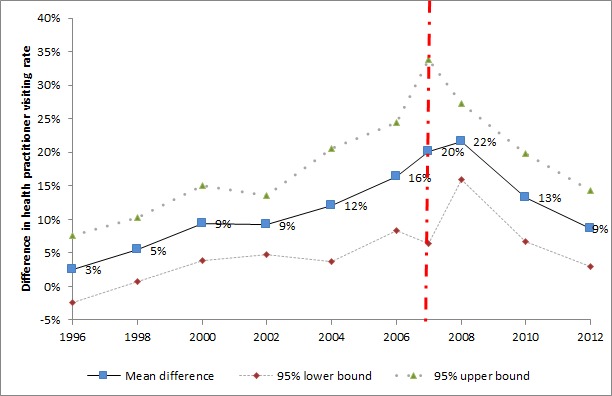
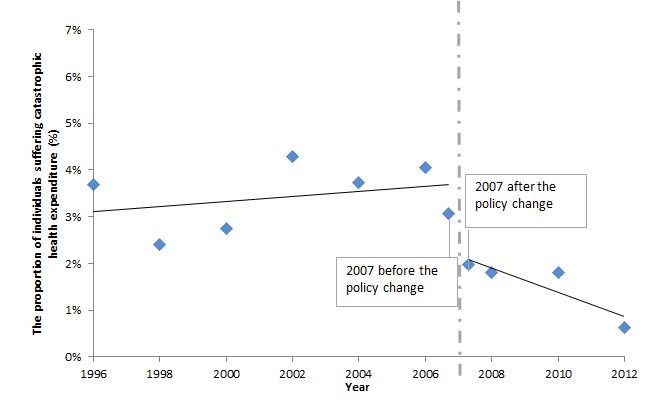
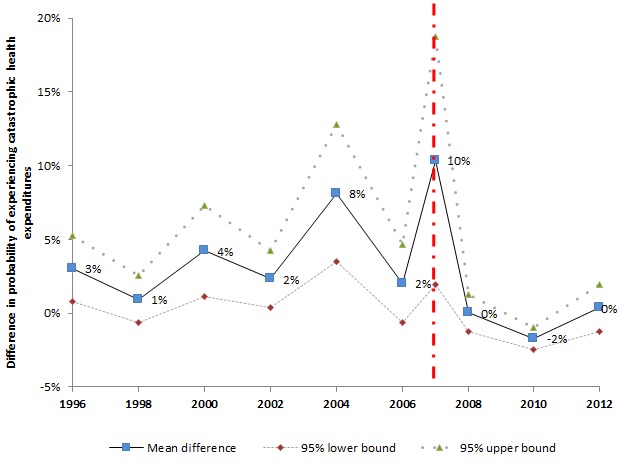
Results: Immediately following the implementation of user-fee-removal, the odds of seeking for health care if the children fell ill in the past 4 weeks increased by 97% (odds ratio 2.0, 95% confidence interval (CI) 1.1 to 3.5, P = 0.018). In the short-term (2007-2008), health care utilization increased at a faster rate among children not in poverty than children in poverty; while this gap narrowed after 2008. There was minimal difference in health care utilization across wealth groups in the medium- to long-term. The household's financial burden (health expenditure as a share of household's non-food expenditures) reduced by 6 percentage points (95% CI: -11 to -1, P = 0.020) right after the policy was implemented and kept at a low level. The difference in financial burden between children in poverty and children not in poverty shrunk rapidly after 2007 and remained small in subsequent years.
Conclusions: User-fee-removal had a positive impact on promoting health care utilization among children and reducing their household health expenditures in Jamaica. The short-term and the medium- to long-term results have different indications: In the short-term, the policy deteriorated the equity of access to health care for children, while the equity status improved fast in the medium- to long-term.
Conflict of interest statement
Competing interests: The authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflict of interest.
Figures
Similar articles
-
Immediate and sustained effects of user fee exemption on healthcare utilization among children under five in Burkina Faso: A controlled interrupted time-series analysis.Soc Sci Med. 2017 Apr;179:27-35. doi: 10.1016/j.socscimed.2017.02.027. Epub 2017 Feb 21. Soc Sci Med. 2017. PMID: 28242542
-
Financial burden of raising CSHCN: association with state policy choices.Pediatrics. 2009 Dec;124 Suppl 4:S435-42. doi: 10.1542/peds.2009-1255P. Pediatrics. 2009. PMID: 19948610
-
Disparities in the financial burden of children's healthcare expenditures.Arch Pediatr Adolesc Med. 2005 Nov;159(11):1008-13. doi: 10.1001/archpedi.159.11.1008. Arch Pediatr Adolesc Med. 2005. PMID: 16275788
-
To retain or remove user fees?: reflections on the current debate in low- and middle-income countries.Appl Health Econ Health Policy. 2006;5(3):137-53. doi: 10.2165/00148365-200605030-00001. Appl Health Econ Health Policy. 2006. PMID: 17132029 Review.
-
What are the economic consequences for households of illness and of paying for health care in low- and middle-income country contexts?Soc Sci Med. 2006 Feb;62(4):858-65. doi: 10.1016/j.socscimed.2005.07.001. Epub 2005 Aug 15. Soc Sci Med. 2006. PMID: 16099574 Review.
Cited by
-
Migration and investments in the health of children left behind: the role of remittances in children's healthcare utilization in Cambodia.Health Policy Plan. 2019 Nov 1;34(9):684-693. doi: 10.1093/heapol/czz076. Health Policy Plan. 2019. PMID: 31539036 Free PMC article.
-
An Evaluation of Healthcare Use and Child Morbidity 4 Years After User Fee Removal in Rural Burkina Faso.Matern Child Health J. 2019 Jun;23(6):777-786. doi: 10.1007/s10995-018-02694-0. Matern Child Health J. 2019. PMID: 30580393 Free PMC article.
-
Comparative Analysis of Healthcare Quality Between the University Hospital of the West Indies and Public Hospitals in Jamaica.Cureus. 2024 Nov 11;16(11):e73423. doi: 10.7759/cureus.73423. eCollection 2024 Nov. Cureus. 2024. PMID: 39664149 Free PMC article.
-
Home visits versus fixed-site care by community health workers and child survival: a cluster-randomized trial, Mali.Bull World Health Organ. 2024 Sep 1;102(9):639-649. doi: 10.2471/BLT.23.290975. Epub 2024 Jun 25. Bull World Health Organ. 2024. PMID: 39219760 Free PMC article. Clinical Trial.
-
Examining vulnerability and resilience in maternal, newborn and child health through a gender lens in low-income and middle-income countries: a scoping review.BMJ Glob Health. 2022 Apr;7(4):e007426. doi: 10.1136/bmjgh-2021-007426. BMJ Glob Health. 2022. PMID: 35443936 Free PMC article.
References
-
- John EU. The impacts of user fees on health services in sub-Saharan African countries: a criticical analysis of the evidence. Am J Public Health Res. 2013;1:196–202. doi: 10.12691/ajphr-1-8-1. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
