

Can pay-for-performance to primary care providers stimulate appropriate use of antibiotics?
- PMID: 28685902
- PMCID: PMC5836891
- DOI: 10.1002/hec.3535
Can pay-for-performance to primary care providers stimulate appropriate use of antibiotics?
Abstract
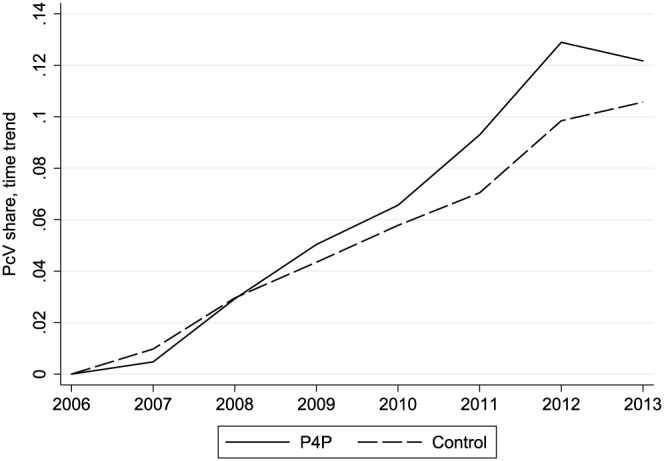
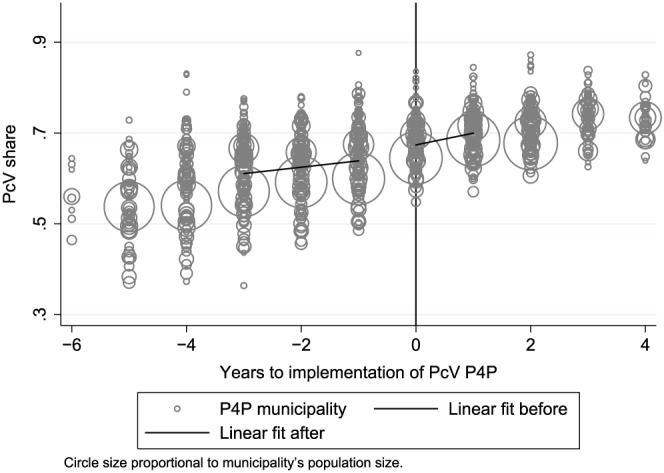
Antibiotic resistance is a major threat to public health worldwide. As the healthcare sector's use of antibiotics is an important contributor to the development of resistance, it is crucial that physicians only prescribe antibiotics when needed and that they choose narrow-spectrum antibiotics, which act on fewer bacteria types, when possible. Inappropriate use of antibiotics is nonetheless widespread, not least for respiratory tract infections (RTI), a common reason for antibiotics prescriptions. We examine if pay-for-performance (P4P) presents a way to influence primary care physicians' choice of antibiotics. During 2006-2013, 8 Swedish healthcare authorities adopted P4P to make physicians select narrow-spectrum antibiotics more often in the treatment of children with RTI. Exploiting register data on all purchases of RTI antibiotics in a difference-in-differences analysis, we find that P4P significantly increased the share of narrow-spectrum antibiotics. There are no signs that physicians gamed the system by issuing more prescriptions overall.
Keywords: antibiotic resistance; pay-for-performance; primary care.
© 2017 The Authors Health Economics Published by John Wiley & Sons Ltd.
Figures
Similar articles
-
Reduction in antibiotic prescribing for respiratory tract infections in Swedish primary care- a retrospective study of electronic patient records.BMC Infect Dis. 2016 Nov 25;16(1):709. doi: 10.1186/s12879-016-2018-9. BMC Infect Dis. 2016. PMID: 27887585 Free PMC article.
-
Antibiotic management of children with infectious diseases in Dutch Primary Care.Fam Pract. 2017 Apr 1;34(2):169-174. doi: 10.1093/fampra/cmw125. Fam Pract. 2017. PMID: 28122841
-
Financial strategies targeting healthcare providers to promote the prudent use of antibiotics: a systematic review of the evidence.Int J Antimicrob Agents. 2021 Dec;58(6):106446. doi: 10.1016/j.ijantimicag.2021.106446. Epub 2021 Oct 2. Int J Antimicrob Agents. 2021. PMID: 34610457
-
Antibiotic prescribing in public and private practice: a cross-sectional study in primary care clinics in Malaysia.BMC Infect Dis. 2016 May 17;16:208. doi: 10.1186/s12879-016-1530-2. BMC Infect Dis. 2016. PMID: 27188538 Free PMC article.
-
Interventions to reduce inappropriate prescribing of antibiotics for acute respiratory tract infections: summary and update of a systematic review.J Int Med Res. 2018 Aug;46(8):3337-3357. doi: 10.1177/0300060518782519. Epub 2018 Jul 1. J Int Med Res. 2018. PMID: 29962311 Free PMC article.
Cited by
-
Can Private Provision of Primary Care Contribute to the Spread of Antibiotic Resistance? A Study of Antibiotic Prescription in Sweden.Pharmacoecon Open. 2021 Jun;5(2):187-195. doi: 10.1007/s41669-020-00234-7. Epub 2020 Oct 23. Pharmacoecon Open. 2021. PMID: 33098069 Free PMC article.
-
Reconsidering performance management to support innovative changes in health care services.J Health Organ Manag. 2024 Mar 22;38(9):125-142. doi: 10.1108/JHOM-12-2022-0379. J Health Organ Manag. 2024. PMID: 38546186 Free PMC article. Review.
-
Effects of pay-for-performance based antimicrobial stewardship on antimicrobial consumption and expenditure: An interrupted time series analysis.Heliyon. 2024 Jun 8;10(12):e32750. doi: 10.1016/j.heliyon.2024.e32750. eCollection 2024 Jun 30. Heliyon. 2024. PMID: 38975216 Free PMC article.
-
GPs' Perspective on a Multimodal Intervention to Enhance Guideline-Adherence in Uncomplicated Urinary Tract Infections: A Qualitative Process Evaluation of the Multicentric RedAres Cluster-Randomised Controlled Trial.Antibiotics (Basel). 2023 Nov 24;12(12):1657. doi: 10.3390/antibiotics12121657. Antibiotics (Basel). 2023. PMID: 38136690 Free PMC article.
-
Fifteen years with patient choice and free establishment in Swedish primary healthcare: what do we know?Scand J Public Health. 2022 Nov;50(7):852-863. doi: 10.1177/14034948221095365. Epub 2022 May 20. Scand J Public Health. 2022. PMID: 35596549 Free PMC article. Review.
References
-
- André, M., Vernby, A. , Odenholt, I. , Lundborg, C. S. , Axelsson, I. , Eriksson, M. , ... Mölstad, S . (2008). Diagnosis‐prescribing surveys in 2000, 2002 and 2005 in Swedish general practice: Consultations, diagnosis, diagnostics and treatment choices. Scandinavian Journal of Infectious Diseases, 40(8), 648–654. - PubMed
-
- Anell, A. , Glenngård, A. H. , & Merkur, S. (2012a). Sweden: Health system review. Health Systems in Transition, 14(5), 1–159. - PubMed
-
- Anell, A. (2015). The public–private pendulum – Patient choice and equity in Sweden. New England Journal of Medicine, 372(1), 1–4. - PubMed
-
- Anell, A. , Nylinder, P. , & Glenngård, A. (2012b). Vårdval i primärvården: Jämförelse av uppdrag, ersättningsprinciper och kostnadsansvar. Stockholm: Sveriges Kommuner och Landsting.
-
- Angrist, J. D. , & Pischke, J.‐S. (2008). Mostly harmless econometrics (1st ed) Princeton: Princeton University Press.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
