

Evaluating phecodes, clinical classification software, and ICD-9-CM codes for phenome-wide association studies in the electronic health record
- PMID: 28686612
- PMCID: PMC5501393
- DOI: 10.1371/journal.pone.0175508
Evaluating phecodes, clinical classification software, and ICD-9-CM codes for phenome-wide association studies in the electronic health record
Abstract
Objective: To compare three groupings of Electronic Health Record (EHR) billing codes for their ability to represent clinically meaningful phenotypes and to replicate known genetic associations. The three tested coding systems were the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, the Agency for Healthcare Research and Quality Clinical Classification Software for ICD-9-CM (CCS), and manually curated "phecodes" designed to facilitate phenome-wide association studies (PheWAS) in EHRs.
Methods and materials: We selected 100 disease phenotypes and compared the ability of each coding system to accurately represent them without performing additional groupings. The 100 phenotypes included 25 randomly-chosen clinical phenotypes pursued in prior genome-wide association studies (GWAS) and another 75 common disease phenotypes mentioned across free-text problem lists from 189,289 individuals. We then evaluated the performance of each coding system to replicate known associations for 440 SNP-phenotype pairs.
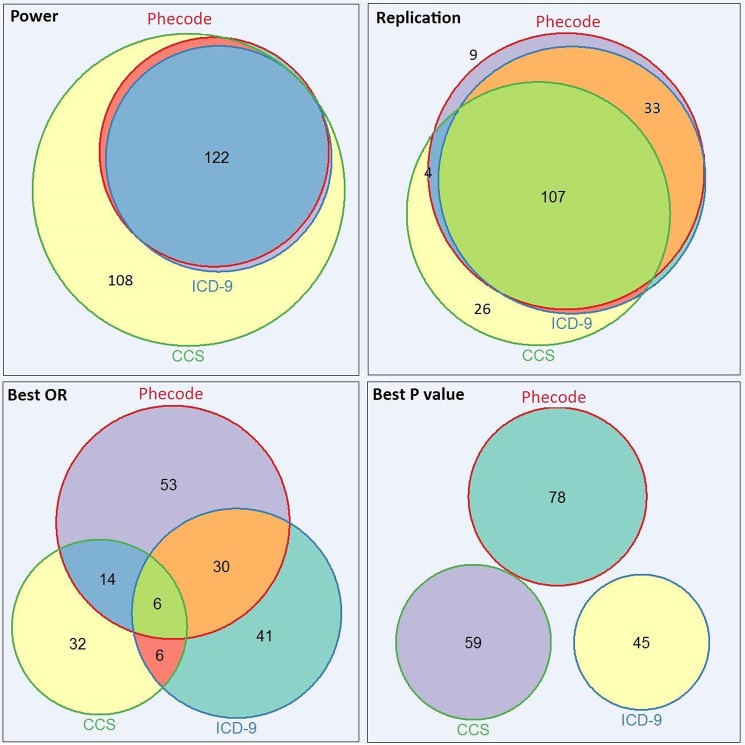
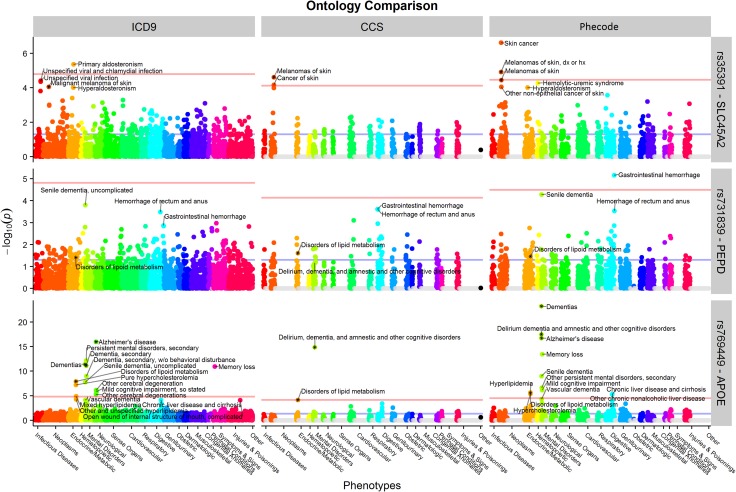
Results: Out of the 100 tested clinical phenotypes, phecodes exactly matched 83, compared to 53 for ICD-9-CM and 32 for CCS. ICD-9-CM codes were typically too detailed (requiring custom groupings) while CCS codes were often not granular enough. Among 440 tested known SNP-phenotype associations, use of phecodes replicated 153 SNP-phenotype pairs compared to 143 for ICD-9-CM and 139 for CCS. Phecodes also generally produced stronger odds ratios and lower p-values for known associations than ICD-9-CM and CCS. Finally, evaluation of several SNPs via PheWAS identified novel potential signals, some seen in only using the phecode approach. Among them, rs7318369 in PEPD was associated with gastrointestinal hemorrhage.
Conclusion: Our results suggest that the phecode groupings better align with clinical diseases mentioned in clinical practice or for genomic studies. ICD-9-CM, CCS, and phecode groupings all worked for PheWAS-type studies, though the phecode groupings produced superior results.
Conflict of interest statement
Figures
References
-
- Roden DM, Xu H, Denny JC, Wilke RA. Electronic medical records as a tool in clinical pharmacology: opportunities and challenges. Clinical pharmacology and therapeutics. 2012;91(6):1083–86. Epub 2012/04/27. doi: 10.1038/clpt.2012.42 ; PubMed Central PMCID: PMC3819803. - DOI - PMC - PubMed
-
- Wilke RA, Xu H, Denny JC, Roden DM, Krauss RM, McCarty CA, et al. The emerging role of electronic medical records in pharmacogenomics. Clinical pharmacology and therapeutics. 2011;89(3):379–86. Epub 2011/01/21. doi: 10.1038/clpt.2010.260 ; PubMed Central PMCID: PMC3204342. - DOI - PMC - PubMed
-
- Bowton E, Field JR, Wang S, Schildcrout JS, Van Driest SL, Delaney JT, et al. Biobanks and electronic medical records: enabling cost-effective research. Science translational medicine. 2014;6(234):234cm3 Epub 2014/05/03. doi: 10.1126/scitranslmed.3008604 . - DOI - PMC - PubMed
-
- Kohane IS. Using electronic health records to drive discovery in disease genomics. Nature reviews Genetics. 2011;12(6):417–28. Epub 2011/05/19. doi: 10.1038/nrg2999 . - DOI - PubMed
-
- Hersh WR, Weiner MG, Embi PJ, Logan JR, Payne PR, Bernstam EV, et al. Caveats for the use of operational electronic health record data in comparative effectiveness research. Medical care. 2013;51(8 Suppl 3):S30–7. Epub 2013/06/19. doi: 10.1097/MLR.0b013e31829b1dbd ; PubMed Central PMCID: PMC3748381. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
