

The rural pipeline to longer-term rural practice: General practitioners and specialists
- PMID: 28686628
- PMCID: PMC5501522
- DOI: 10.1371/journal.pone.0180394
The rural pipeline to longer-term rural practice: General practitioners and specialists
Abstract
Background: Rural medical workforce shortage contributes to health disadvantage experienced by rural communities worldwide. This study aimed to determine the regional results of an Australian Government sponsored national program to enhance the Australian rural medical workforce by recruiting rural background students and establishing rural clinical schools (RCS). In particular, we wished to determine predictors of graduates' longer-term rural practice and whether the predictors differ between general practitioners (GPs) and specialists.
Methods: A cross-sectional cohort study, conducted in 2012, of 729 medical graduates of The University of Queensland 2002-2011. The outcome of interest was primary place of graduates' practice categorised as rural for at least 50% of time since graduation ('Longer-term Rural Practice', LTRP) among GPs and medical specialists. The main exposures were rural background (RB) or metropolitan background (MB), and attendance at a metropolitan clinical school (MCS) or the Rural Clinical School for one year (RCS-1) or two years (RCS-2).
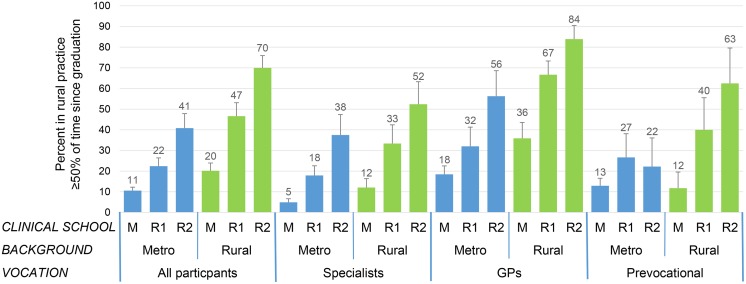
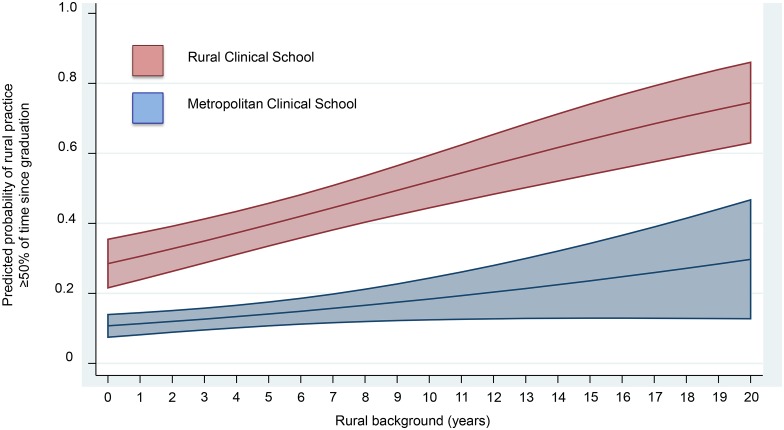
Results: Independent predictors of LTRP (odds ratio [95% confidence interval]) were RB (2.10 [1.37-3.20]), RCS-1 (2.85 [1.77-4.58]), RCS-2 (5.38 [3.15-9.20]), GP (3.40 [2.13-5.43]), and bonded scholarship (2.11 [1.19-3.76]). Compared to being single, having a metropolitan background partner was a negative predictor (0.34 [0.21-0.57]). The effects of RB and RCS were additive-compared to MB and MCS (Reference group): RB and RCS-1 (6.58[3.32-13.04]), RB and RCS-2 (10.36[4.89-21.93]). Although specialists were less likely than GPs to be in LTRP, the pattern of the effects of rural exposures was similar, although some significant differences in the effects of the duration of RCS attendance, bonded scholarships and partner's background were apparent.
Conclusions: Among both specialists and GPs, rural background and rural clinical school attendance are independent, duration-dependent, and additive, predictors of longer-term rural practice. Metropolitan-based medical schools can enhance both specialist and GP rural medical workforce by enrolling rural background medical students and providing them with long-term rural undergraduate clinical training. Policy settings to achieve optimum rural workforce outcomes may differ between specialists and GPs.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Increasing access to health workers in remote and rural areas through improved retention: global policy recommendations. Geneva: World Health Organisation; 2010. - PubMed
-
- Rourke J. How can medical schools contribute to the education, recruitment and retention of rural physicians in their region? Bull World Health Organ. 2010;88:395–396. doi: 10.2471/BLT.09.073072 - DOI - PMC - PubMed
-
- Australian Institute of Health and Welfare (AIHW). Australian Burden of Disease Study: fatal burden of disease in Aboriginal and Torres Strait Islander people 2010. Australian Burden of Disease Study series no. 2. Cat. no. BOD 2. Canberra: AIHW 2015. (http://www.aihw.gov.au/publication-detail/?id=60129550618). [Accessed 5 February 2016].
-
- Grobler L, Marais BJ, Mabunda S. Interventions for increasing the proportion of health professionals practising in rural and other underserved areas. Cochrane Database Syst Rev. 2015. June 30; (6):CD005314 doi: 10.1002/14651858.CD005314.pub3 - DOI - PMC - PubMed
-
- Dolea C, Stormont L, Braichet JM. Evaluated strategies to increase attraction and retention of health workers in remote and rural areas. Bull World Health Organ. 2010; 88 (5):379–85. doi: 10.2471/BLT.09.070607 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
