

Immunohistochemical identification of Propionibacterium acnes in granuloma and inflammatory cells of myocardial tissues obtained from cardiac sarcoidosis patients
- PMID: 28686683
- PMCID: PMC5501515
- DOI: 10.1371/journal.pone.0179980
Immunohistochemical identification of Propionibacterium acnes in granuloma and inflammatory cells of myocardial tissues obtained from cardiac sarcoidosis patients
Abstract
Background: Although rare, cardiac sarcoidosis (CS) is potentially fatal. Early diagnosis and intervention are essential, but histopathologic diagnosis is limited. We aimed to detect Propionibacterium acnes, a commonly implicated etiologic agent of sarcoidosis, in myocardial tissues obtained from CS patients.
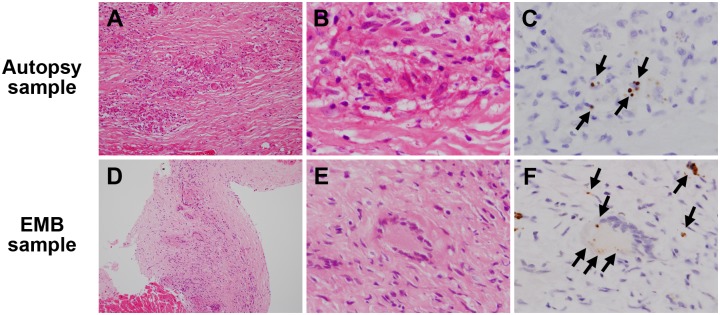
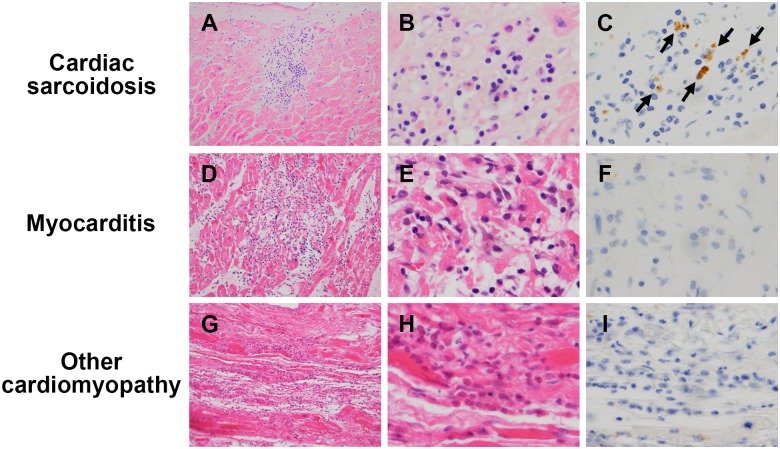
Methods and results: We examined formalin-fixed paraffin-embedded myocardial tissues obtained by surgery or autopsy and endomyocardial biopsy from patients with CS (n = 26; CS-group), myocarditis (n = 15; M-group), or other cardiomyopathies (n = 39; CM-group) using immunohistochemistry (IHC) with a P. acnes-specific monoclonal antibody. We found granulomas in 16 (62%) CS-group samples. Massive (≥14 inflammatory cells) and minimal (<14 inflammatory cells) inflammatory foci, respectively, were detected in 16 (62%) and 11 (42%) of the CS-group samples, 10 (67%) and 10 (67%) of the M-group samples, and 1 (3%) and 18 (46%) of the CM-group samples. P. acnes-positive reactivity in granulomas, massive inflammatory foci, and minimal inflammatory foci were detected in 10 (63%), 10 (63%), and 8 (73%) of the CS-group samples, respectively, and in none of the M-group and CM-group samples.
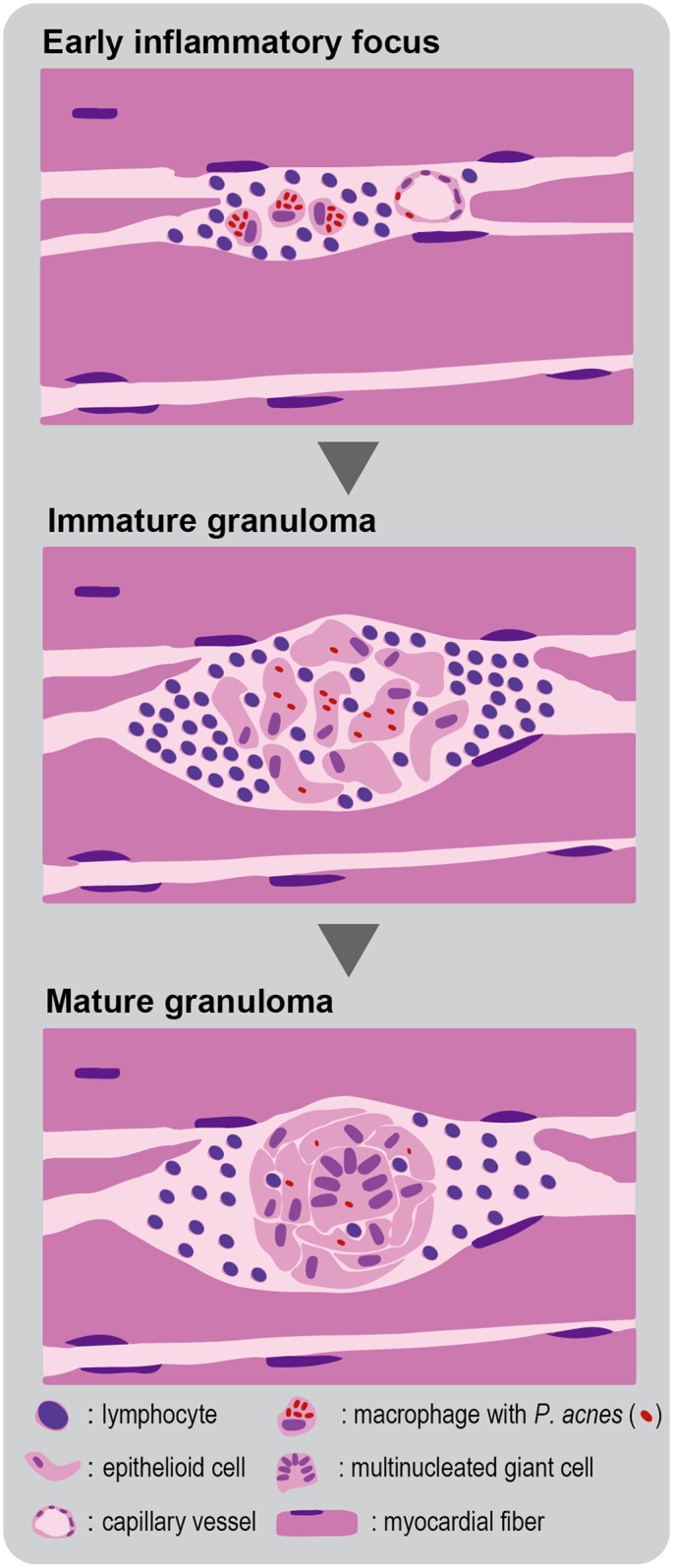
Conclusions: Frequent identification of P. acnes in sarcoid granulomas of originally aseptic myocardial tissues suggests that this indigenous bacterium causes granuloma in many CS patients. IHC detection of P. acnes in massive or minimal inflammatory foci of myocardial biopsy samples without granulomas may be useful for differentiating sarcoidosis from myocarditis or other cardiomyopathies.
Conflict of interest statement
Figures

References
-
- Sekhri V, Sanal S, Delorenzo LJ, Aronow WS, Maguire GP. Cardiac sarcoidosis: a comprehensive review. Arch Med Sci. 2011;7(4):546–54. Epub 2012/02/01. doi: 10.5114/aoms.2011.24118 ; - DOI - PMC - PubMed
-
- Iwai K, Tachibana T, Takemura T, Matsui Y, Kitaichi M, Kawabata Y. Pathological studies on sarcoidosis autopsy. I. Epidemiological features of 320 cases in Japan. Acta pathologica japonica. 1993;43(7–8):372–6. Epub 1993/07/01. . - PubMed
-
- Silverman KJ, Hutchins GM, Bulkley BH. Cardiac sarcoid: a clinicopathologic study of 84 unselected patients with systemic sarcoidosis. Circulation. 1978;58(6):1204–11. Epub 1978/12/01. . - PubMed
-
- Nagai T, Nagano N, Sugano Y, Asaumi Y, Aiba T, Kanzaki H, et al. Effect of Corticosteroid Therapy on Long-Term Clinical Outcome and Left Ventricular Function in Patients With Cardiac Sarcoidosis. Circ J. 2015;79(7):1593–600. doi: 10.1253/circj.CJ-14-1275 . - DOI - PubMed
-
- Chiu CZ, Nakatani S, Zhang G, Tachibana T, Ohmori F, Yamagishi M, et al. Prevention of left ventricular remodeling by long-term corticosteroid therapy in patients with cardiac sarcoidosis. The American journal of cardiology. 2005;95(1):143–6. Epub 2004/12/28. doi: 10.1016/j.amjcard.2004.08.083 . - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
