

Association of neuron-specific enolase values with outcomes in cardiac arrest survivors is dependent on the time of sample collection
- PMID: 28687073
- PMCID: PMC5501942
- DOI: 10.1186/s13054-017-1766-2
Association of neuron-specific enolase values with outcomes in cardiac arrest survivors is dependent on the time of sample collection
Abstract
Background: Despite marked advances in intensive cardiology care, current options for outcome prediction in cardiac arrest survivors remain significantly limited. The aim of our study was, therefore, to compare the day-specific association of neuron-specific enolase (NSE) with outcomes in out-of-hospital cardiac arrest (OHCA) survivors treated with hypothermia.
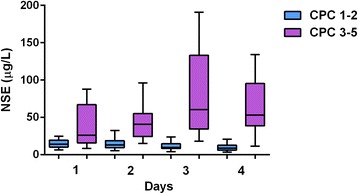
Methods: Eligible patients were OHCA survivors treated with targeted temperature management at 33 °C for 24 h using an endovascular device. Blood samples for NSE levels measurement were drawn on days 1, 2, 3, and 4 after hospital admission. Thirty-day neurological outcomes according to the Cerebral Performance Category (CPC) scale and 12-month mortality were evaluated as clinical end points.
Results: A total of 153 cardiac arrest survivors (mean age 64.2 years) were enrolled in the present study. Using ROC analysis, optimal cutoff values of NSE for prediction of CPC 3-5 score on specific days were determined as: day 1 > 20.4 mcg/L (sensitivity 63.3%; specificity 82.1%; P = 0.002); day 2 > 29.0 mcg/L (72.5%; 94.4%; P < 0.001); and day 3 > 20.7 mcg/L (94.4%; 86.7%; P < 0.001). The highest predictive value, however, was observed on day 4 > 19.4 mcg/L (93.5%; 91.0%; P < 0.001); NSE value >50.2 mcg/L at day 4 was associated with poor outcome with 100% specificity and 42% sensitivity. Moreover, NSE levels measured on all individual days also predicted 12-month mortality (P < 0.001); the highest predictive value for death was observed on day 3 > 18.1 mcg/L (85.3%; 72.0%; P < 0.001). Significant association with prognosis was found also for changes in NSE at different time points. An NSE level on day 4 > 20.0 mcg/L, together with a change > 0.0 mcg/L from day 3 to day 4, predicted poor outcome (CPC 3-5) with 100% specificity and 73% sensitivity.
Conclusions: Our results suggest that NSE levels are a useful tool for predicting 30-day neurological outcome and long-term mortality in OHCA survivors treated with targeted temperature management at 33 °C. The highest associations of NSE with outcomes were observed on day 4 and day 3 after cardiac arrest.
Keywords: Cardiac arrest; Mild hypothermia; Neuron-specific enolase; Prognosis.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Institutional Ethics Committee of the Na Homolce Hospital (Prague, Czech Republic). Surviving patients with favorable neurological outcomes, and family members of deceased subjects or individuals with unfavorable neurological outcomes provided informed consent retrospectively. Blood samples drawn from patients who were not willing to participate in the study (expressed by family members in cases involving deceased relatives or those with unfavorable neurological outcomes) were discarded and the clinical data were not used in the analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



Similar articles
-
Change in neuron specific enolase levels in out-of-hospital cardiopulmonary arrest survivors as a simple and useful tool to predict neurological prognosis.Rev Esp Cardiol (Engl Ed). 2020 Mar;73(3):232-240. doi: 10.1016/j.rec.2019.01.007. Epub 2019 Mar 30. Rev Esp Cardiol (Engl Ed). 2020. PMID: 30935900 English, Spanish.
-
Serum neutrophil gelatinase-associated lipocalin levels predict the neurological outcomes of out-of-hospital cardiac arrest victims.BMC Cardiovasc Disord. 2017 May 8;17(1):111. doi: 10.1186/s12872-017-0545-y. BMC Cardiovasc Disord. 2017. PMID: 28482803 Free PMC article.
-
Changes in neuron-specific enolase are more suitable than its absolute serum levels for the prediction of neurologic outcome in hypothermia-treated patients with out-of-hospital cardiac arrest.Neurocrit Care. 2014 Jun;20(3):358-66. doi: 10.1007/s12028-013-9848-8. Neurocrit Care. 2014. PMID: 23836424
-
Serum Neuron-Specific Enolase Thresholds for Predicting Postcardiac Arrest Outcome: A Systematic Review and Meta-analysis.Neurology. 2022 Jan 4;98(1):e62-e72. doi: 10.1212/WNL.0000000000012967. Epub 2021 Oct 18. Neurology. 2022. PMID: 34663643
-
The utility of brain biomarkers in predicting survival and neurological outcomes in pediatric patients after cardiac arrest: A systematic review and meta-analysis.Cardiol J. 2025;32(2):130-141. doi: 10.5603/cj.103883. Epub 2025 Mar 10. Cardiol J. 2025. PMID: 40062924 Free PMC article.
Cited by
-
Using Out-of-Hospital Cardiac Arrest (OHCA) and Cardiac Arrest Hospital Prognosis (CAHP) Scores with Modified Objective Data to Improve Neurological Prognostic Performance for Out-of-Hospital Cardiac Arrest Survivors.J Clin Med. 2021 Apr 22;10(9):1825. doi: 10.3390/jcm10091825. J Clin Med. 2021. PMID: 33922191 Free PMC article.
-
ICU 'Magic Numbers': The Role of Biomarkers in Supporting Clinical Decision-Making.Diagnostics (Basel). 2025 Apr 11;15(8):975. doi: 10.3390/diagnostics15080975. Diagnostics (Basel). 2025. PMID: 40310334 Free PMC article. Review.
-
Targeted Temperature Management Suppresses Hypoxia-Inducible Factor-1α and Vascular Endothelial Growth Factor Expression in a Pig Model of Cardiac Arrest.Neurocrit Care. 2021 Oct;35(2):379-388. doi: 10.1007/s12028-020-01166-0. Epub 2021 Jan 5. Neurocrit Care. 2021. PMID: 33403582 Free PMC article.
-
European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care.Intensive Care Med. 2021 Apr;47(4):369-421. doi: 10.1007/s00134-021-06368-4. Epub 2021 Mar 25. Intensive Care Med. 2021. PMID: 33765189 Free PMC article.
-
The use of neurone specific enolase to prognosticate neurological recovery and long term neurological outcomes in OOHCA patients.J Intensive Care Soc. 2023 Nov;24(4):386-391. doi: 10.1177/17511437231160089. Epub 2023 Jun 29. J Intensive Care Soc. 2023. PMID: 37841299 Free PMC article.
References
-
- Grasner JT, Lefering R, Koster RW, Masterson S, Bottiger BW, Herlitz J, Wnent J, Tjelmeland IB, Ortiz FR, Maurer H, et al. EuReCa ONE-27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation. 2016;105:188–95. doi: 10.1016/j.resuscitation.2016.06.004. - DOI - PubMed
-
- Callaway CW, Donnino MW, Fink EL, Geocadin RG, Golan E, Kern KB, Leary M, Meurer WJ, Peberdy MA, Thompson TM, et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S465–482. doi: 10.1161/CIR.0000000000000262. - DOI - PMC - PubMed
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Bottiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79(3):350–79. doi: 10.1016/j.resuscitation.2008.09.017. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
