

Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: a single-centre, randomised, controlled, phase 3 trial
- PMID: 28687375
- PMCID: PMC5560102
- DOI: 10.1016/S1470-2045(17)30414-X
Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: a single-centre, randomised, controlled, phase 3 trial
Erratum in
-
Correction to Lancet Oncol 2017; 18: 1040-48.Lancet Oncol. 2017 Aug;18(8):e433. doi: 10.1016/S1470-2045(17)30530-2. Epub 2017 Jul 26. Lancet Oncol. 2017. PMID: 28759379 No abstract available.
-
Correction to Lancet Oncol 2017; 18: 1040-48.Lancet Oncol. 2017 Sep;18(9):e510. doi: 10.1016/S1470-2045(17)30636-8. Lancet Oncol. 2017. PMID: 28884700 No abstract available.
Abstract
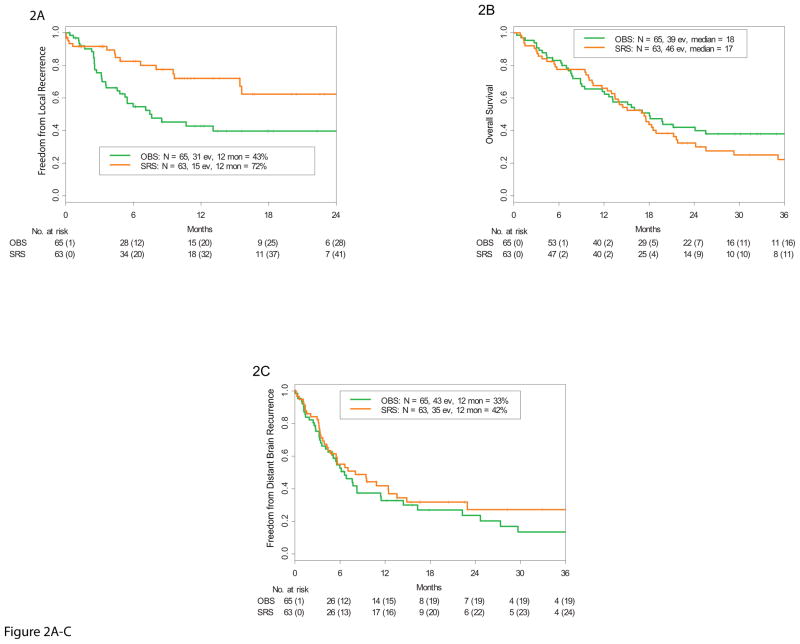
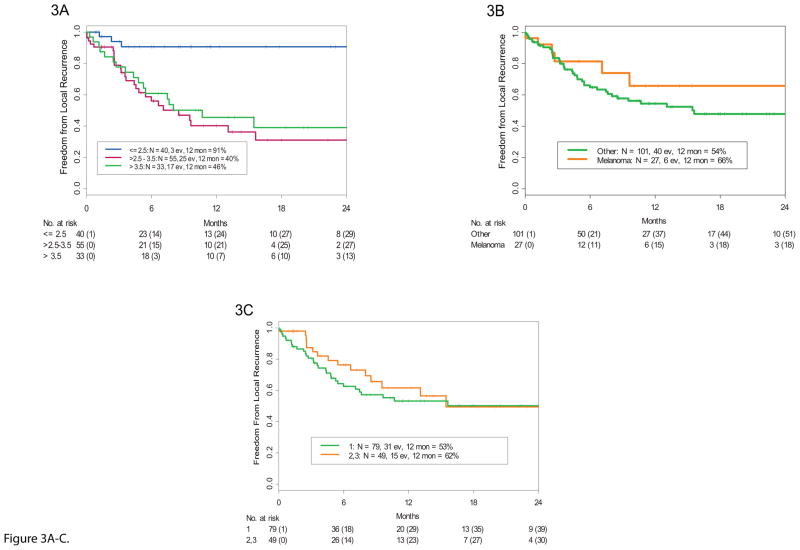
Background: After brain metastasis resection, whole brain radiotherapy decreases local recurrence, but might cause cognitive decline. We did this study to determine if stereotactic radiosurgery (SRS) to the surgical cavity improved time to local recurrence compared with that for surgical resection alone.
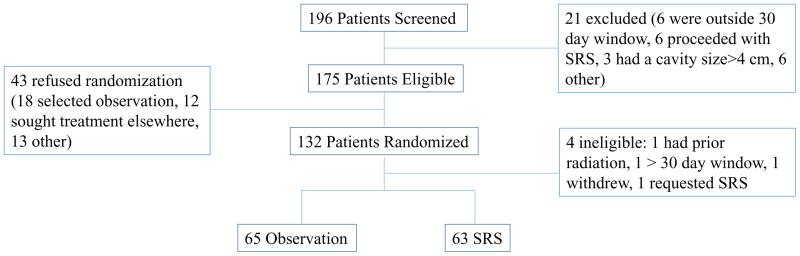
Methods: In this randomised, controlled, phase 3 trial, we recruited patients at a single tertiary cancer centre in the USA. Eligible patients were older than 3 years, had a Karnofsky Performance Score of 70 or higher, were able to have an MRI scan, and had a complete resection of one to three brain metastases (with a maximum diameter of the resection cavity ≤4 cm). Patients were randomly assigned (1:1) with a block size of four to either SRS of the resection cavity (within 30 days of surgery) or observation. Patients were stratified by histology of the primary tumour, metastatic tumour size, and number of metastases. The primary endpoint was time to local recurrence in the resection cavity, assessed by blinded central review of brain MRI scans by the study neuroradiologist in the modified intention-to-treat population that analysed patients by randomised allocation but excluded patients found ineligible after randomisation. Participants and other members of the treatment team (excluding the neuroradiologist) were not masked to treatment allocation. The trial is registered with ClinicalTrials.gov, number NCT00950001, and is closed to new participants.
Findings: Between Aug 13, 2009, and Feb 16, 2016, 132 patients were randomly assigned to the observation group (n=68) or SRS group (n=64), with 128 patients available for analysis; four patients were ineligible (three from the SRS group and one from the observation group). Median follow-up was 11·1 months (IQR 4·8-20·4). 12-month freedom from local recurrence was 43% (95% CI 31-59) in the observation group and 72% (60-87) in the SRS group (hazard ratio 0·46 [95% CI 0·24-0·88]; p=0·015). There were no adverse events or treatment-related deaths in either group.
Interpretation: SRS of the surgical cavity in patients who have had complete resection of one, two, or three brain metastases significantly lowers local recurrence compared with that noted for observation alone. Thus, the use of SRS after brain metastasis resection could be an alternative to whole-brain radiotherapy.
Funding: National Institutes of Health.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declared no conflicts of interest
Figures
Comment in
-
Radiosurgery for resected brain metastases-a new standard of care?Lancet Oncol. 2017 Aug;18(8):985-987. doi: 10.1016/S1470-2045(17)30448-5. Epub 2017 Jul 4. Lancet Oncol. 2017. PMID: 28687374 No abstract available.
-
[Reconsideration of radiosurgery for resection cavities following complete resection of 1-3 brain metastases].Strahlenther Onkol. 2017 Dec;193(12):1074-1076. doi: 10.1007/s00066-017-1210-1. Strahlenther Onkol. 2017. PMID: 28887615 German. No abstract available.
-
Control versus cognition: the changing paradigm of adjuvant therapy for resected brain metastasis.Neuro Oncol. 2018 Jan 10;20(1):2-3. doi: 10.1093/neuonc/nox180. Neuro Oncol. 2018. PMID: 29126327 Free PMC article. No abstract available.
-
Stereotactic Radiosurgery for Resected Brain Metastases: New Evidence Supports a Practice Shift, but Questions Remain.Int J Radiat Oncol Biol Phys. 2018 Mar 1;100(3):535-538. doi: 10.1016/j.ijrobp.2017.08.024. Int J Radiat Oncol Biol Phys. 2018. PMID: 29413262 No abstract available.
References
-
- Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med. 1990;322(8):494–500. - PubMed
-
- Patchell RA, Tibbs PA, Regine WF, et al. Postoperative radiotherapy in the treatment of single metastases to the brain: a randomized trial. Jama. 1998;280(17):1485–9. - PubMed
-
- Chang EL, Wefel JS, Hess KR, et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. The Lancet Oncology. 2009;10(11):1037–44. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
