

SMD Kozlowski type caused by p.Arg594His substitution in TRPV4 reveals abnormal ossification and notochordal remnants in discs and vertebrae
- PMID: 28687525
- PMCID: PMC5785083
- DOI: 10.1016/j.ejmg.2017.07.004
SMD Kozlowski type caused by p.Arg594His substitution in TRPV4 reveals abnormal ossification and notochordal remnants in discs and vertebrae
Abstract
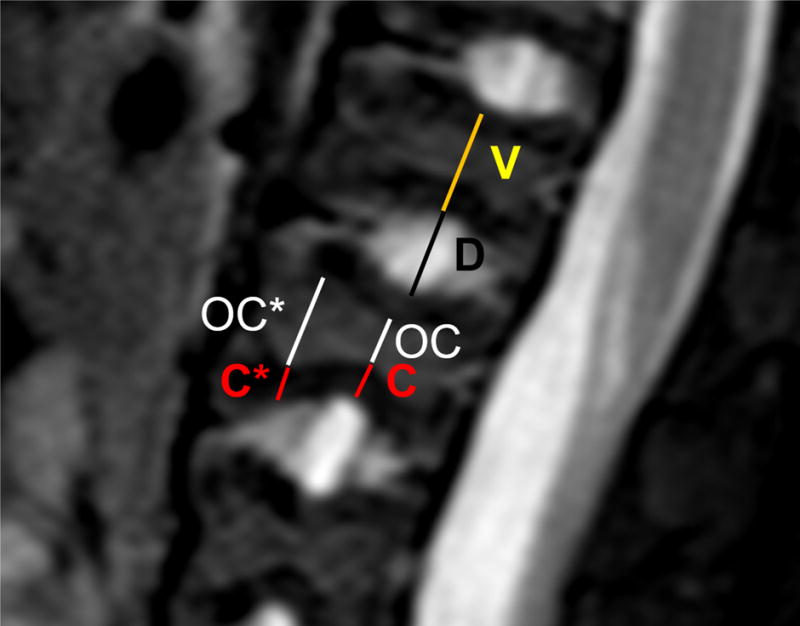
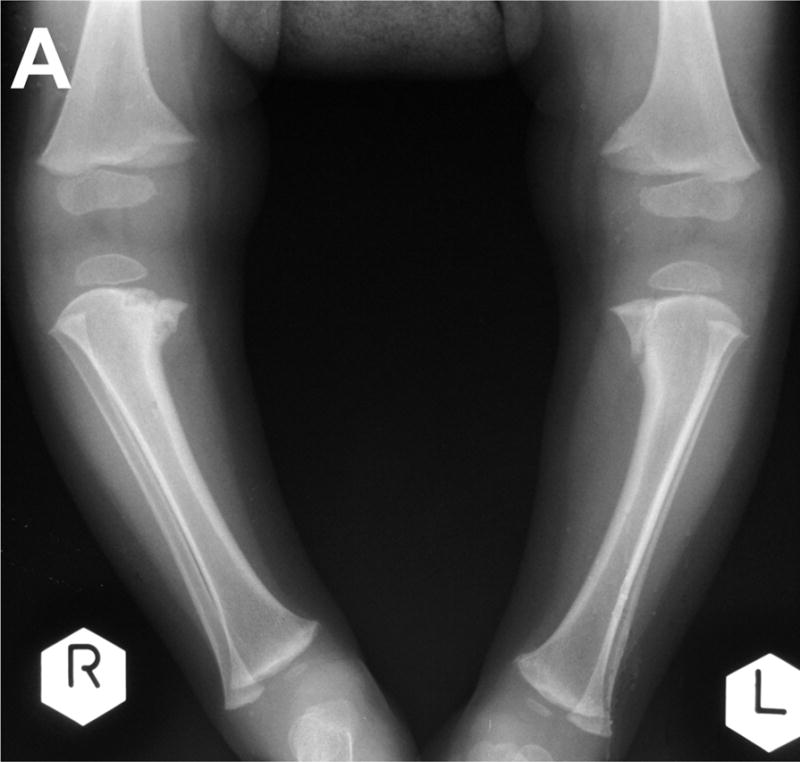
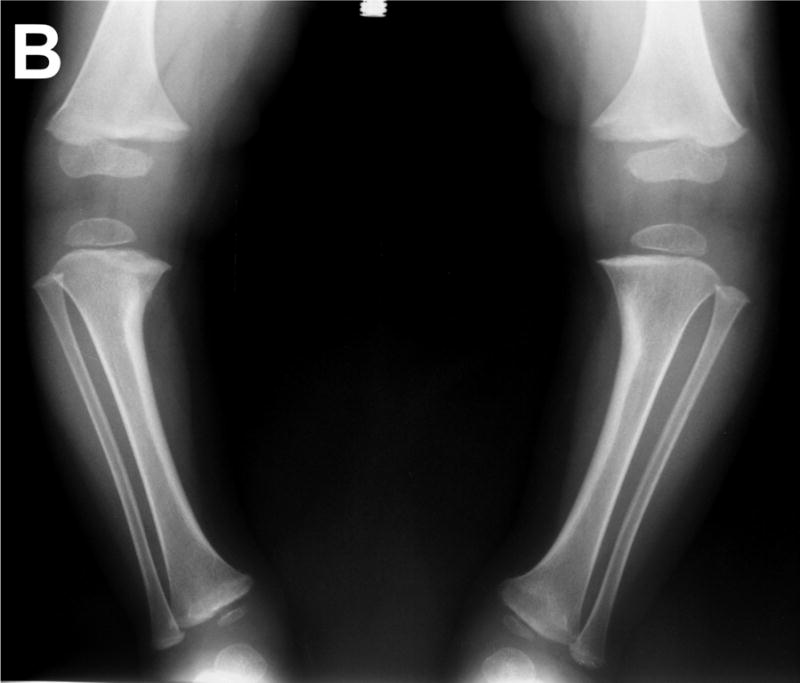
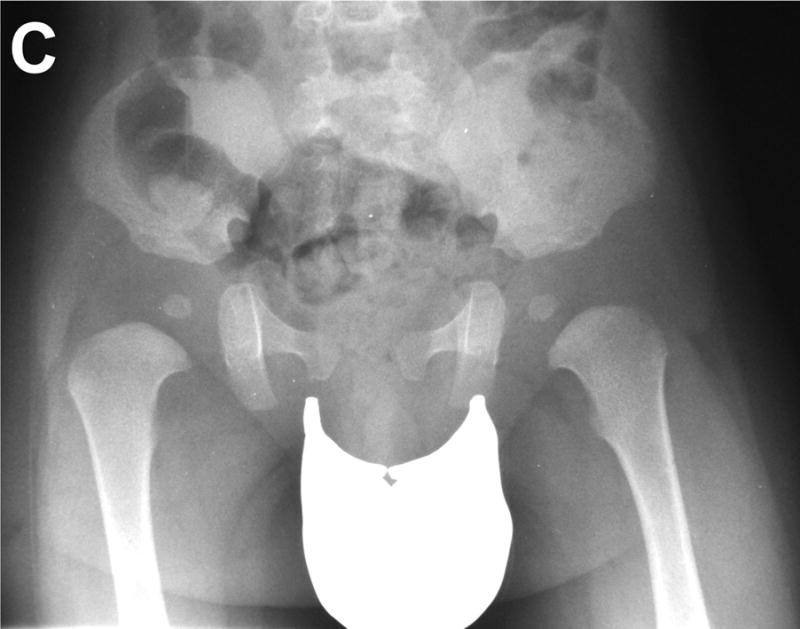
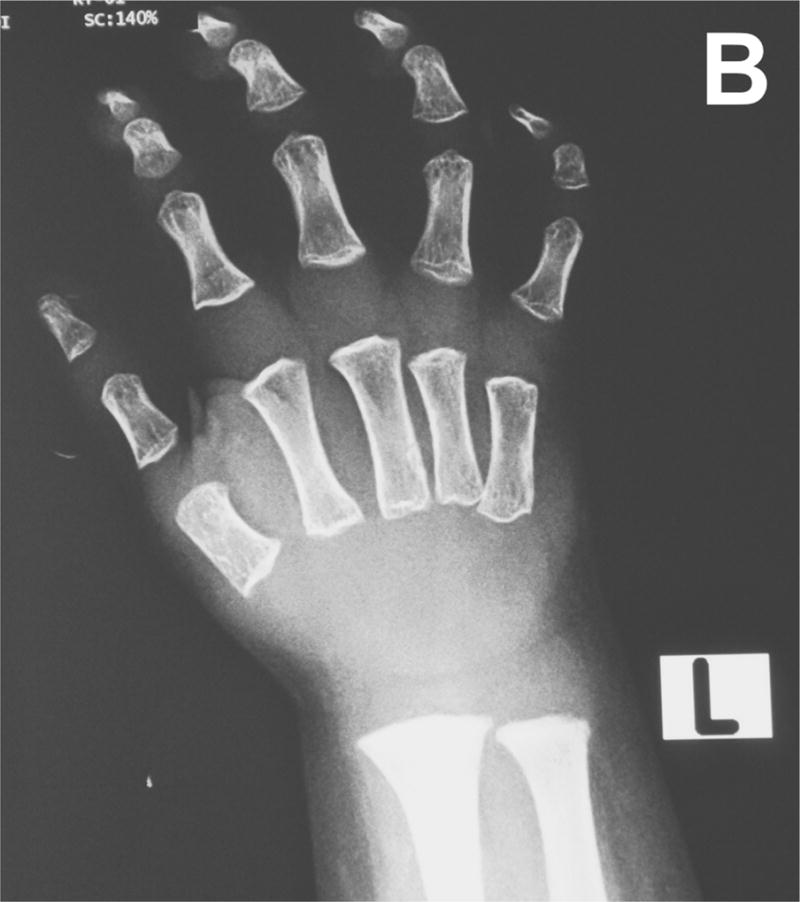
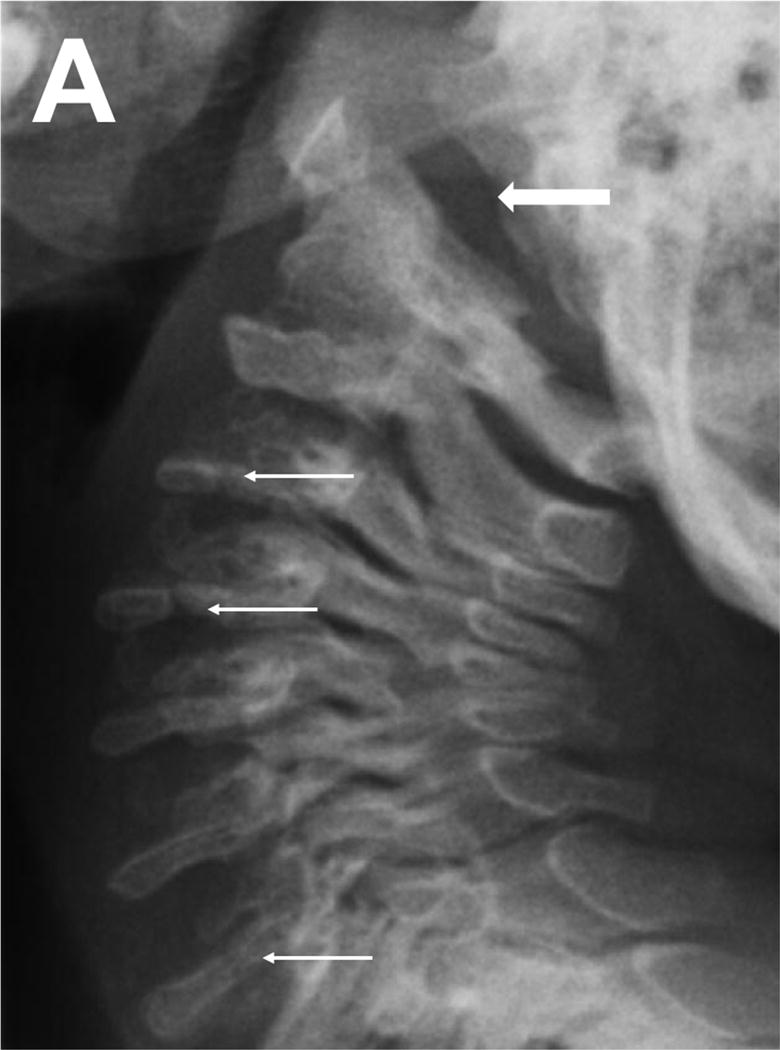
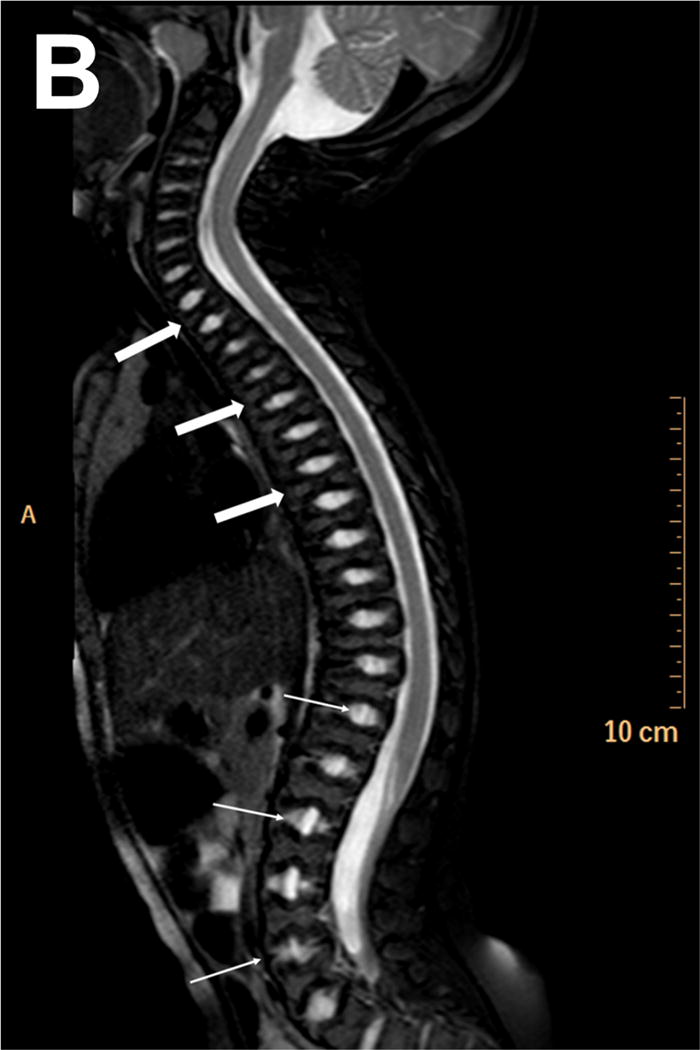
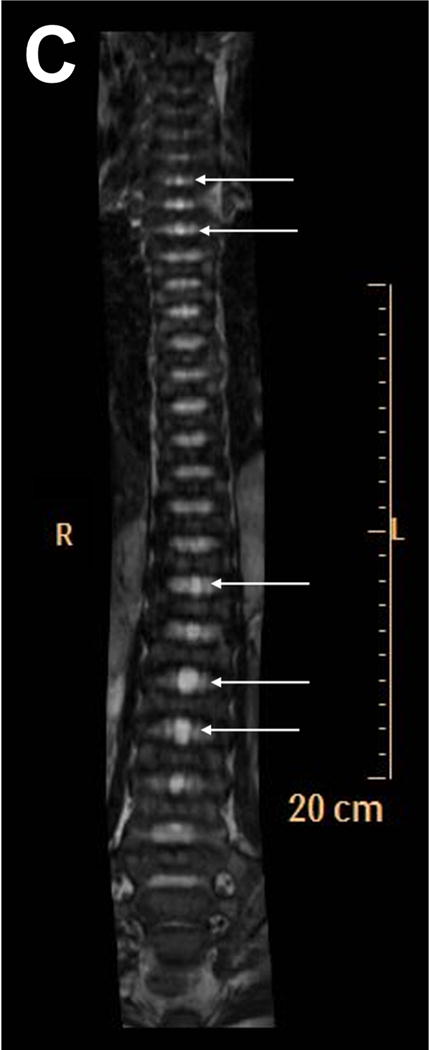
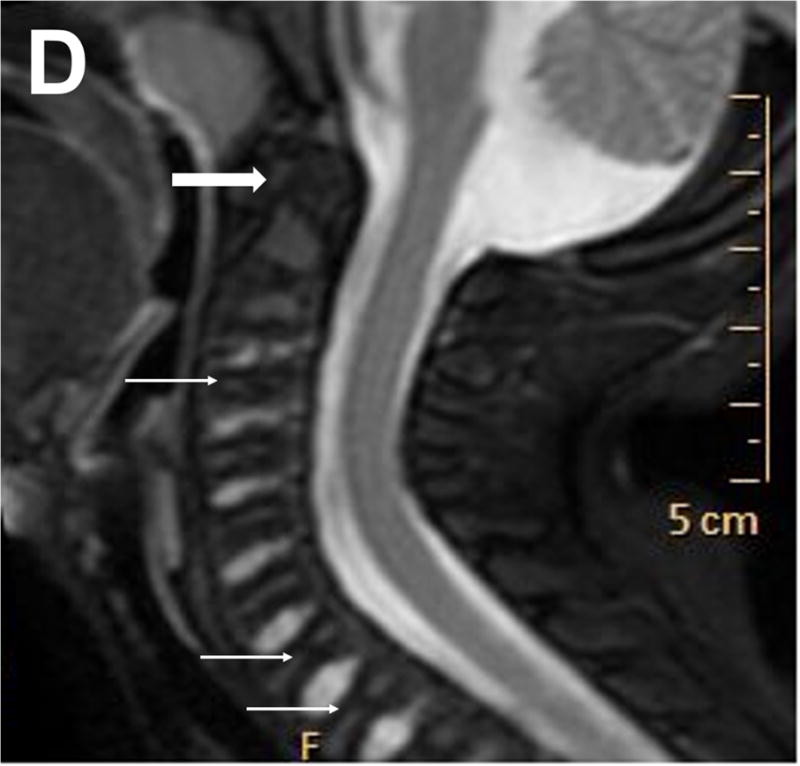
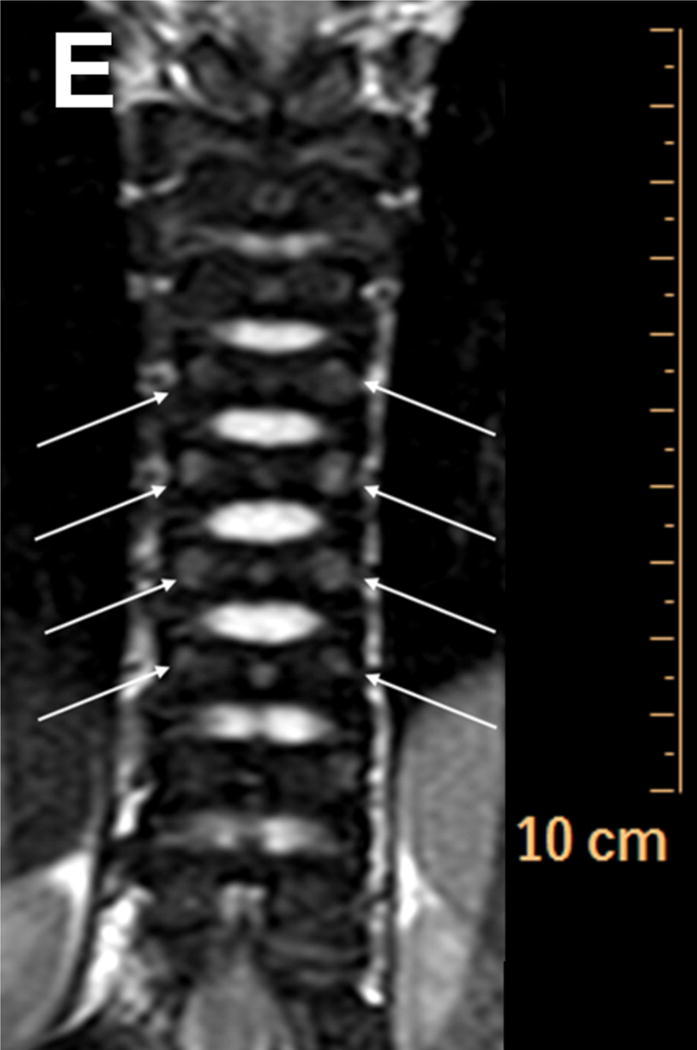
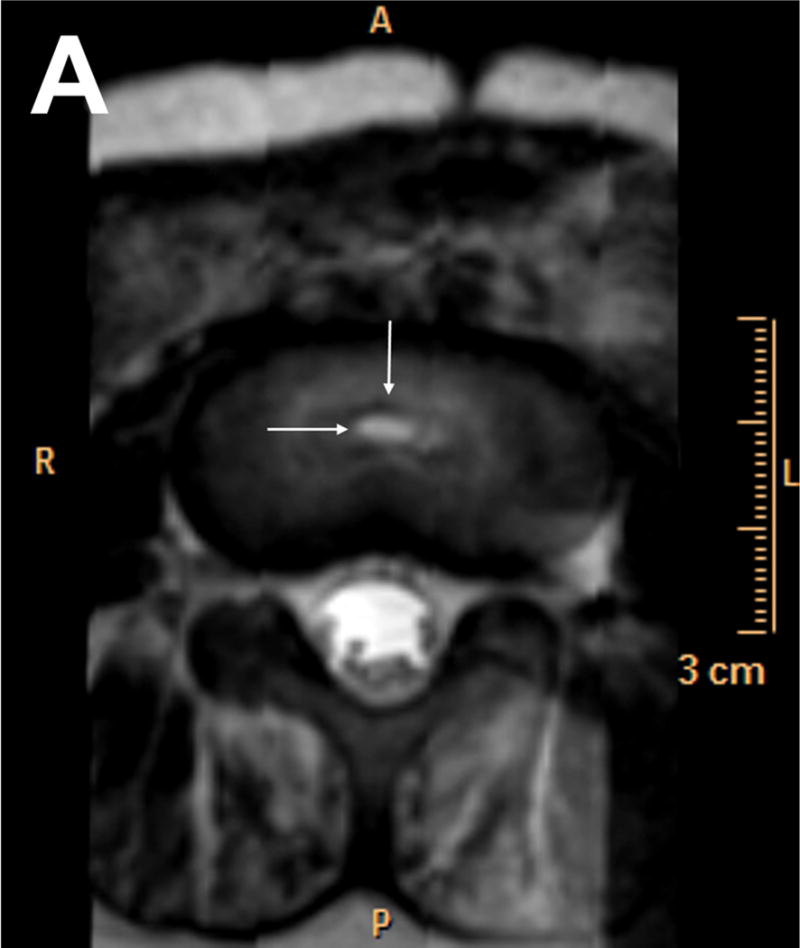
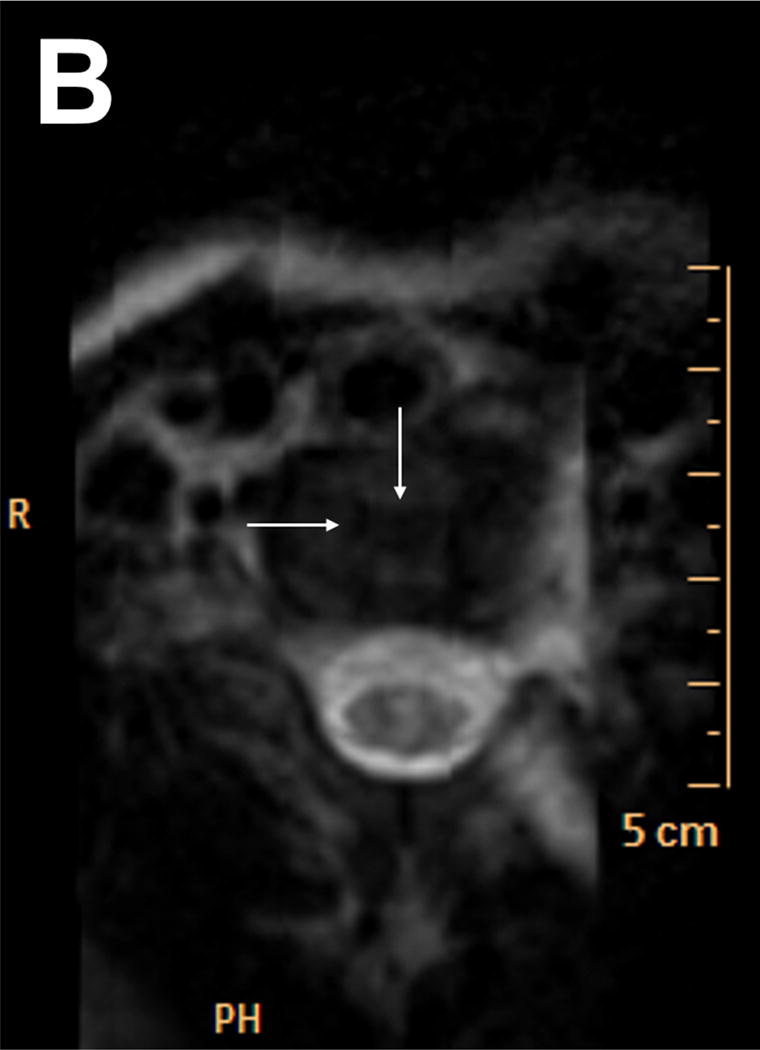
Spondylometaphyseal dysplasia Kozlowski type (SMDK) is a monogenic disorder within the TRPV4 dysplasia spectrum and has characteristic spinal and metaphyseal changes. We report skeletal MR imaging in a two-year-old patient who manifested typical clinical and radiographic features of SMDK. The diagnosis was confirmed by molecular analysis which revealed a mutation NM_021625.4:c.1781G > A - p.(Arg594His) in exon 11 of the TRPV4 gene. We have documented abnormalities in endochondral formation of the long and short tubular bones as well as round bones of the wrists and feet. The vertebral bodies had increased thickness of hyaline cartilage which enveloped ossification centers. The vertebrae and discs also had abnormalities in size, shape and structure. These anomalies were most likely the consequence of notochordal remnants presence within the intervertebral discs and in the vertebral bodies. The advantages of MR imaging in bone dysplasias caused by TRPV4 mutations are emphasized in this article.
Copyright © 2017 Elsevier Masson SAS. All rights reserved.
Conflict of interest statement
The authors declare that they have no competing financial interests.
Figures




Similar articles
-
Comparison of the natural course of clinical and radiologic features in 13 patients with TRPV4-related skeletal dysplasias.Pediatr Radiol. 2025 Mar;55(3):505-519. doi: 10.1007/s00247-024-06145-7. Epub 2025 Jan 18. Pediatr Radiol. 2025. PMID: 39825918
-
Mutations in the gene encoding the calcium-permeable ion channel TRPV4 produce spondylometaphyseal dysplasia, Kozlowski type and metatropic dysplasia.Am J Hum Genet. 2009 Mar;84(3):307-15. doi: 10.1016/j.ajhg.2009.01.021. Epub 2009 Feb 19. Am J Hum Genet. 2009. PMID: 19232556 Free PMC article.
-
Novel and recurrent TRPV4 mutations and their association with distinct phenotypes within the TRPV4 dysplasia family.J Med Genet. 2010 Oct;47(10):704-9. doi: 10.1136/jmg.2009.075358. Epub 2010 Jun 24. J Med Genet. 2010. PMID: 20577006
-
Human skeletal dysplasia caused by a constitutive activated transient receptor potential vanilloid 4 (TRPV4) cation channel mutation.Exp Mol Med. 2012 Dec 31;44(12):707-22. doi: 10.3858/emm.2012.44.12.080. Exp Mol Med. 2012. PMID: 23143559 Free PMC article. Review.
-
The importance of conventional radiography in the mutational analysis of skeletal dysplasias (the TRPV4 mutational family).Pediatr Radiol. 2012 Jan;42(1):15-23. doi: 10.1007/s00247-011-2229-6. Epub 2011 Aug 24. Pediatr Radiol. 2012. PMID: 21863289 Review.
Cited by
-
Comparison of the natural course of clinical and radiologic features in 13 patients with TRPV4-related skeletal dysplasias.Pediatr Radiol. 2025 Mar;55(3):505-519. doi: 10.1007/s00247-024-06145-7. Epub 2025 Jan 18. Pediatr Radiol. 2025. PMID: 39825918
References
-
- Andreucci E, Aftimos S, Alcausin M, Haan E, Hunter W, Kannu P, Kerr B, McGillivray G, Gardner RJM, Patricelli MG, Sillence D, Thompson E, Zacharin M, Zankl A, Lamandé SR, Savarirayan R. TRPV4 related skeletal dysplasias: a phenotypic spectrum highlighted by clinical, radiographic, and molecular studies in 21 new families. Orphanet J Rare Dis. 2011;6:37. - PMC - PubMed
-
- Cho TJ, Matsumoto K, Fano V, Dai J, Kim OH, Chae JH, Yoo WJ, Tanaka Y, Matsui Y, Takigami I, Monges S, Zabel B, Shimizu K, Nishimura G, Lausch E, Ikegawa S. TRPV4-pathy manifesting both skeletal dysplasia and peripheral neuropathy: a report of three patients. Am J Med Genet A. 2012;158A(4):795–802. - PubMed
-
- Christopherson LR, Rabin BM, Hallam DK, Russell EJ. Perisistence of the notochordal canal: MR and plain film appearance. AJNR Am J Neuroradiol. 1999;20:33–36. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
