

Evaluating the Impact and Cost-Effectiveness of Statin Use Guidelines for Primary Prevention of Coronary Heart Disease and Stroke
- PMID: 28687710
- PMCID: PMC5605438
- DOI: 10.1161/CIRCULATIONAHA.117.027067
Evaluating the Impact and Cost-Effectiveness of Statin Use Guidelines for Primary Prevention of Coronary Heart Disease and Stroke
Abstract
Background: Statins are effective in the primary prevention of atherosclerotic cardiovascular disease. The 2013 American College of Cardiology/American Heart Association (ACC/AHA) guideline expands recommended statin use, but its cost-effectiveness has not been compared with other guidelines.
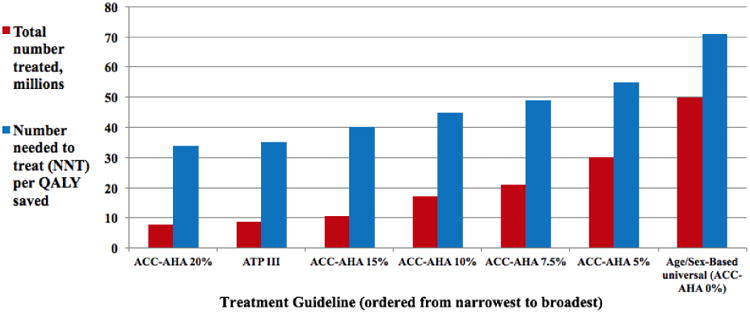
Methods: We used the Cardiovascular Disease Policy Model to estimate the cost-effectiveness of the ACC/AHA guideline relative to current use, Adult Treatment Panel III guidelines, and universal statin use in all men 45 to 74 years of age and women 55 to 74 years of age over a 10-year horizon from 2016 to 2025. Sensitivity analyses varied costs, risks, and benefits. Main outcomes were incremental cost-effectiveness ratios and numbers needed to treat for 10 years per quality-adjusted life-year gained.
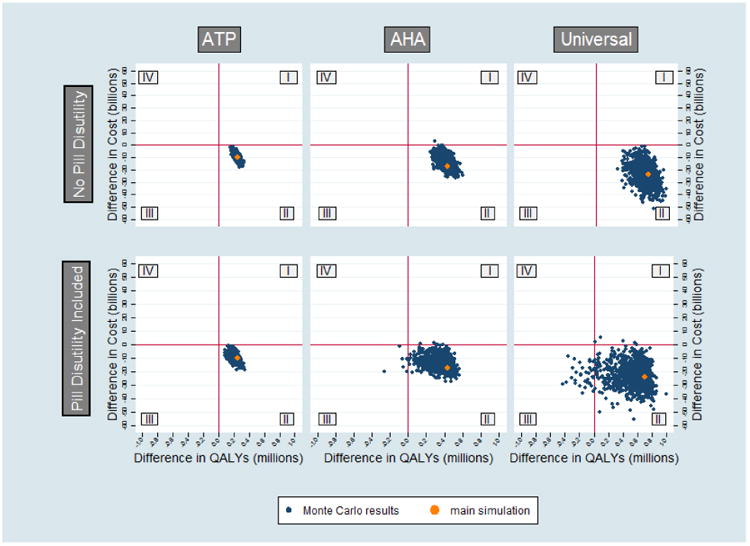
Results: Each approach produces substantial benefits and net cost savings relative to the status quo. Full adherence to the Adult Treatment Panel III guideline would result in 8.8 million more statin users than the status quo, at a number needed to treat for 10 years per quality-adjusted life-year gained of 35. The ACC/AHA guideline would potentially result in up to 12.3 million more statin users than the Adult Treatment Panel III guideline, with a marginal number needed to treat for 10 years per quality-adjusted life-year gained of 68. Moderate-intensity statin use in all men 45 to 74 years of age and women 55 to 74 years of age would result in 28.9 million more statin users than the ACC/AHA guideline, with a marginal number needed to treat for 10 years per quality-adjusted life-year gained of 108. In all cases, benefits would be greater in men than women. Results vary moderately with different risk thresholds for instituting statins and statin toxicity estimates but depend greatly on the disutility caused by daily medication use (pill burden).
Conclusions: At a population level, the ACC/AHA guideline for expanded statin use for primary prevention is projected to treat more people, to save more lives, and to cost less compared with Adult Treatment Panel III in both men and women. Whether individuals benefit from long-term statin use for primary prevention depends more on the disutility associated with pill burden than their degree of cardiovascular risk.
Keywords: coronary disease; cost-benefit analysis; hydroxymethylglutaryl-CoA reductase inhibitors; primary prevention.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
When to Start a Statin Is a Preference-Sensitive Decision.Circulation. 2017 Sep 19;136(12):1099-1101. doi: 10.1161/CIRCULATIONAHA.117.029808. Circulation. 2017. PMID: 28923904 Free PMC article. No abstract available.
References
-
- Global Burden of Disease. World Health Organization; 2004. [Accessed on June 22, 2017]. Projections of mortality and burden of disease 2002–2030. Available from http://www.who.int/topics/global_burden_of_disease/en/
-
- LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart JC, Gotto AM, Greten H, Kastelein JJ, Shepherd J, Wenger NK. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. - PubMed
-
- Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, Voysey M, Gray A, Collins R, Baigent C. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–90. - PMC - PubMed
-
- Engstrom A, Jacob J, Lundin D. Sharp drop in prices after the introduction of generic substitution. Swedish Pharmaceutical Benefits Board (LFN) for the World Health Organization Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policy's Information Network (PPRI); Solna: 2006. Available from http://whocc.goeg.at/
-
- Chalasani N, Aljadhey H, Kesterson J, Murray M, Hall SD. Patients with elevated liver enzymes are not at higher risk for statin hepatotoxicity. Gastroenterology. 2004;126:1287–92. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
