

A meta-analysis on progressive atrophy in intractable temporal lobe epilepsy: Time is brain?
- PMID: 28687722
- PMCID: PMC5539734
- DOI: 10.1212/WNL.0000000000004176
A meta-analysis on progressive atrophy in intractable temporal lobe epilepsy: Time is brain?
Abstract
Objective: It remains unclear whether drug-resistant temporal lobe epilepsy (TLE) is associated with cumulative brain damage, with no expert consensus and no quantitative syntheses of the available evidence.
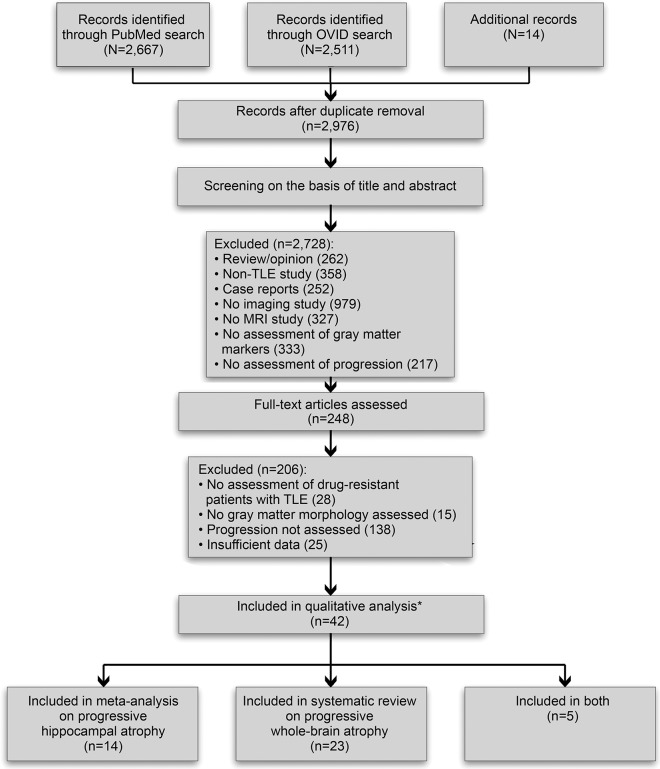
Methods: We conducted a systematic review and meta-analysis of MRI studies on progressive atrophy, searching PubMed and Ovid MEDLINE databases for cross-sectional and longitudinal quantitative MRI studies on drug-resistant TLE.
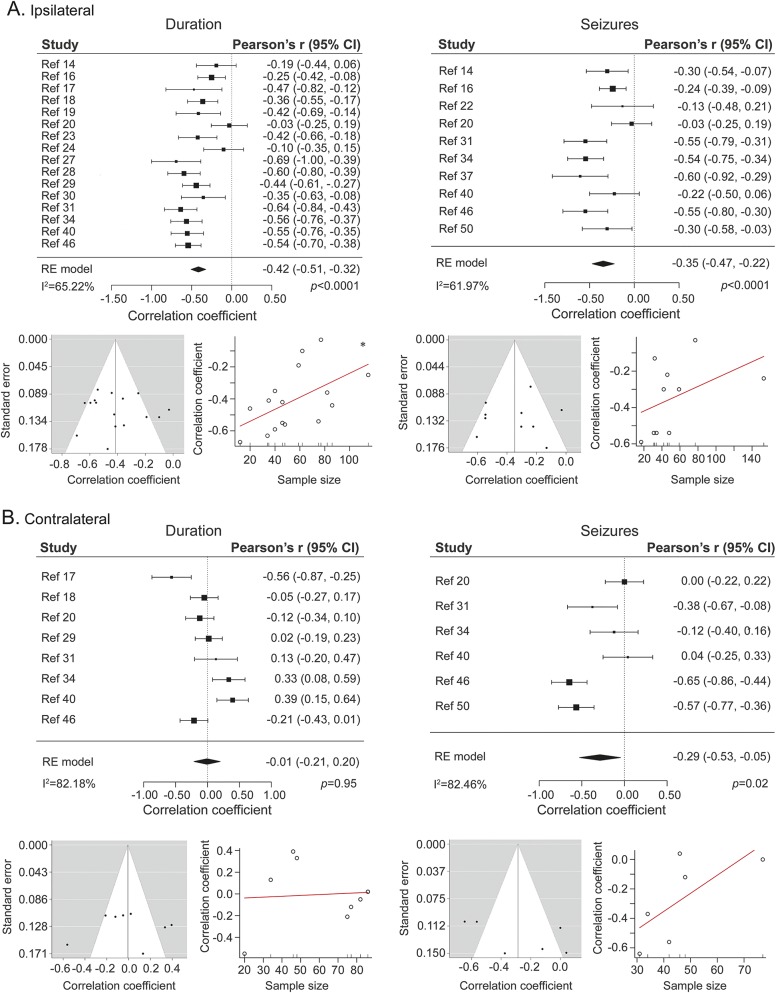
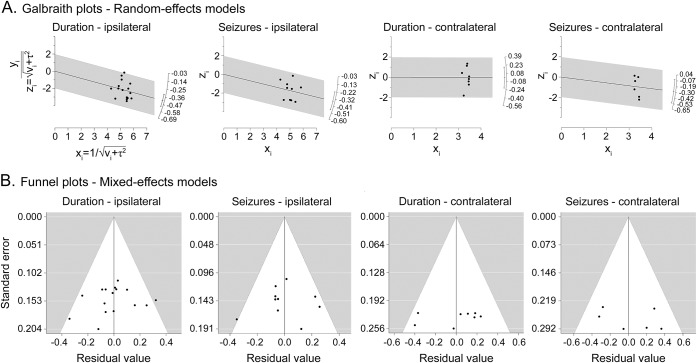
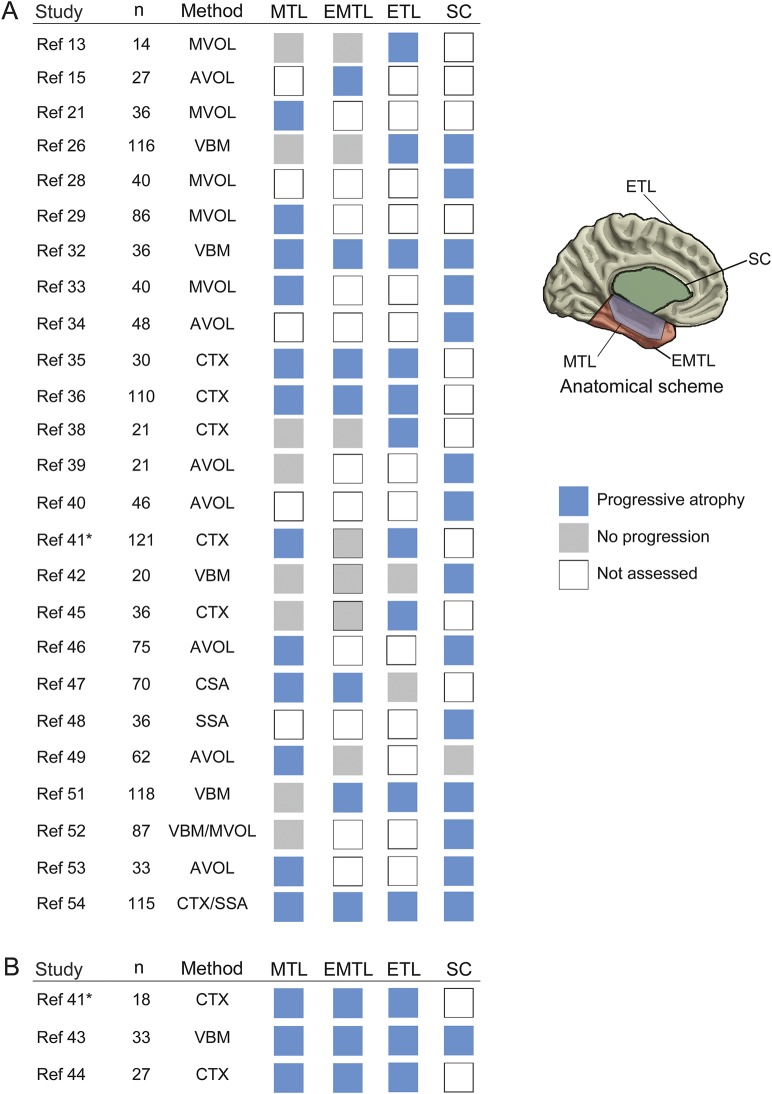
Results: We screened 2,976 records and assessed eligibility of 248 full-text articles. Forty-two articles met the inclusion criteria for quantitative evaluation. We observed a predominance of cross-sectional studies, use of different clinical indices of progression, and high heterogeneity in age-control procedures. Meta-analysis of 18/1 cross-sectional/longitudinal studies on hippocampal atrophy (n = 979 patients) yielded a pooled effect size of r = -0.42 for ipsilateral atrophy related to epilepsy duration (95% confidence interval [CI] -0.51 to -0.32; p < 0.0001; I2 = 65.22%) and r = -0.35 related to seizure frequency (95% CI -0.47 to -0.22; p < 0.0001; I2 = 61.97%). Sensitivity analyses did not change the results. Narrative synthesis of 25/3 cross-sectional/longitudinal studies on whole brain atrophy (n = 1,504 patients) indicated that >80% of articles reported duration-related progression in extratemporal cortical and subcortical regions. Detailed analysis of study design features yielded low to moderate levels of evidence for progressive atrophy across studies, mainly due to dominance of cross-sectional over longitudinal investigations, use of diverse measures of seizure estimates, and absence of consistent age control procedures.
Conclusions: While the neuroimaging literature is overall suggestive of progressive atrophy in drug-resistant TLE, published studies have employed rather weak designs to directly demonstrate it. Longitudinal multicohort studies are needed to unequivocally differentiate aging from disease progression.
© 2017 American Academy of Neurology.
Figures
References
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M; Effectiveness and Efficiency of Surgery for Temporal Lobe Epilepsy Study Group. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med 2001;345:311–318. - PubMed
-
- Wiebe S. Burden of intractable epilepsy. Adv Neurol 2006;97:1–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous