

Pooled Systemic Efficacy and Safety Data from the Pivotal Phase II Studies (NP28673 and NP28761) of Alectinib in ALK-positive Non-Small Cell Lung Cancer
- PMID: 28689043
- PMCID: PMC6886236
- DOI: 10.1016/j.jtho.2017.06.070
Pooled Systemic Efficacy and Safety Data from the Pivotal Phase II Studies (NP28673 and NP28761) of Alectinib in ALK-positive Non-Small Cell Lung Cancer
Abstract
Introduction: Alectinib demonstrated clinical efficacy and an acceptable safety profile in two phase II studies (NP28761 and NP28673). Here we report the pooled efficacy and safety data after 15 and 18 months more follow-up than in the respective primary analyses.
Methods: Enrolled patients had ALK receptor tyrosine kinase gene (ALK)-positive NSCLC and had progressed while taking, or could not tolerate, crizotinib. Patients received oral alectinib, 600 mg twice daily. The primary end point in both studies was objective response rate assessed by an independent review committee (IRC) using the Response Evaluation Criteria in Solid Tumors, version 1.1. Secondary end points included disease control rate, duration of response, progression-free survival, overall survival, and safety.
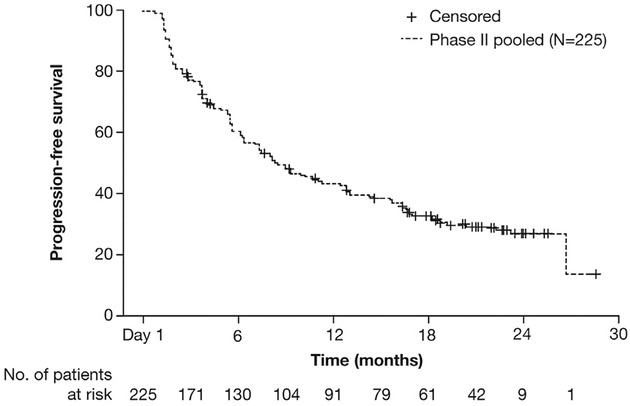
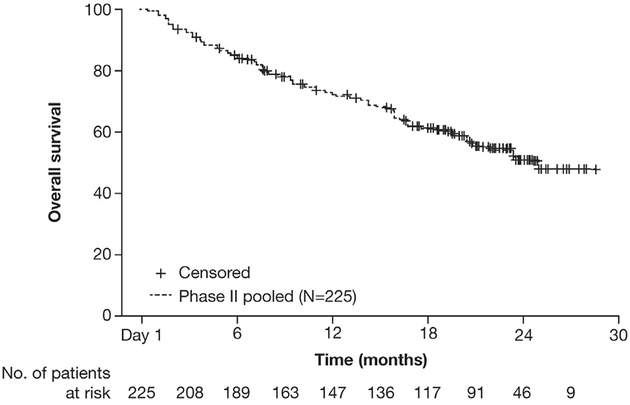
Results: The pooled data set included 225 patients (n = 138 in NP28673 and n = 87 in NP28761). The response-evaluable population included 189 patients (84% [n = 122 in NP28673 and n = 67 in NP28761]). In the response-evaluable population, objective response rate as assessed by the IRC was 51.3% (95% confidence interval [CI]: 44.0-58.6 [all PRs]), the disease control rate was 78.8% (95% CI: 72.3-84.4), and the median duration of response was 14.9 months (95% CI: 11.1-20.4) after 58% of events. Median progression-free survival as assessed by the IRC was 8.3 months (95% CI: 7.0-11.3) and median overall survival was 26.0 months (95% CI: 21.4-not estimable). Grade 3 or higher adverse events (AEs) occurred in 40% of patients, 6% of patients had treatment withdrawn on account of AEs, and 33% had AEs leading to dose interruptions/modification.
Conclusions: This pooled data analysis confirmed the robust systemic efficacy of alectinib in ALK-positive NSCLC with a durable response rate. Alectinib also had an acceptable safety profile with a longer duration of follow-up.
Keywords: Alectinib; NP28673; NP28761; Non–small cell lung cancer; Pooled analysis.
Copyright © 2017 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure: Dr. Yang has received advisory board fees from Boehringer Ingelheim, Bayer, AstraZeneca, Roche/Genentech, Chugai, Clovis Oncology, Eli Lilly, Merck Sharp and Dohme, Merck Serono, Pfizer, Novartis, Celgene, Merrimack, Yuhan Pharmaceuticals, and Daiichi Sankyo. Dr. Ou has received personal fees for Pfizer, AstraZeneca, ARIAD, and Roche outside the submitted work. Dr. De Petris has received personal fees from Roche, AstraZeneca, and Bristol-Myers Squibb. Dr. Gadgeel has received consultancy fees from Boehringer Ingelheim, ARIAD, Novartis, and Genentech. Dr. Gandhi has received consultancy fees from Genentech/Roche, Pfizer, Merck, Abbvie, and AstraZeneca and personal fees from Merck and Bristol-Myers Squibb IION Foundation. Dr. Kim has received personal fees from Roche. Dr. Barlesi has received consulting fees from Roche. Dr. Govindan has received travel accommodation fees and consulting fees from Merck, Boehringer Ingelheim, Celgene, Roche, Stemcentrix, and Abbe Vie and consultancy fees from GlaxoSmithKline, Clovis, and Helsinn Healthcare. Dr. Dingemans has received consultancy fees from Eli Lilly, AstraZeneca, Clovis, Boehringer Ingelheim, and Merck Sharp and Dohme. Dr. Lena reports advisory board membership for Roche, Merck Sharp and Dohme, Bristol-Myers Squibb, Novartis, Pfizer, and AstraZeneca and has been reimbursed for meeting expenses from Roche, Merck Sharp and Dohme, Bristol-Myers Squibb, Lilly, and Amgen. Dr. Popat has received personal fees from Roche, Pfizer, and Novartis outside the submitted work. Dr. Dansin has received personal fees from Bristol-Myers Squibb, AstraZeneca, and Roche. Ms. Golding, Dr. Bordogna, Dr. Balas, Mr. Morcos, and Dr. Zeaiter are employees of and have stock ownership in Roche. Dr. Shaw has received consulting fees from Ignyta and Taiho and advisory board fees from Pfizer, Novartis, Genentech/Roche, Ariad, Daiichi-Sankyo, Blueprint Medicines, Loxo, EMD Serono, and Foundation Medicine. The remaining authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
