

Pathophysiology and Current Clinical Management of Preeclampsia
- PMID: 28689331
- PMCID: PMC5916784
- DOI: 10.1007/s11906-017-0757-7
Pathophysiology and Current Clinical Management of Preeclampsia
Abstract
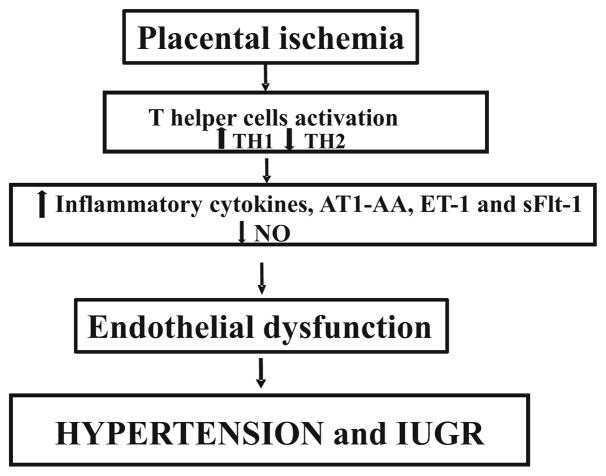
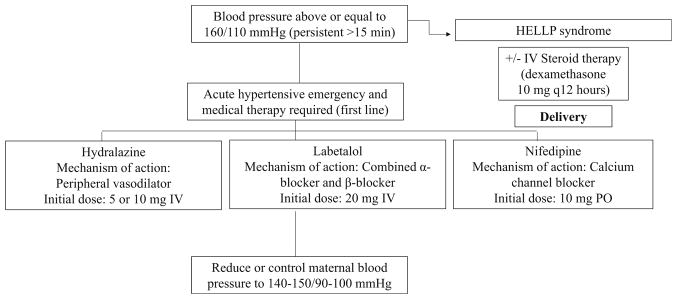
Preeclampsia is characterized by blood pressure greater than 140/90 mmHg in the second half of pregnancy. This disease is a major contributor to preterm and low birth weight babies. The early delivery of the baby, which becomes necessary for maintaining maternal well-being, makes preeclampsia the leading cause for preterm labor and infant mortality and morbidity. Currently, there is no cure for this pregnancy disorder. The current clinical management of PE is hydralazine with labetalol and magnesium sulfate to slow disease progression and prevent maternal seizure, and hopefully prolong the pregnancy. This review will highlight factors implicated in the pathophysiology of preeclampsia and current treatments for the management of this disease.
Keywords: Endothelial dysfunction; Inflammation; Placental ischemia; Preeclampsia.
Figures
References
-
- American College of O Gynecologists, Task Force on Hypertension in P. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstetrics and gynecology. 2013;122(5):1122–31. doi: 10.1097/01.AOG.0000437382.03963.88. This report highlights recommendations and guidelines for the management of patients with hypertension during and after pregnancy. - DOI - PubMed
-
- Creasy RK, Resnik R, Greene MF, Iams JD, Lockwood CJ. Creasy and Resnik’s maternal-fetal medicine: principles and practice. 7
-
- Duley L. Maternal mortality associated with hypertensive disorders of pregnancy in Africa, Asia, Latin America and the Caribbean. Br J Obstet Gynaecol. 1992;99(7):547–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
