

Asthma Exacerbations: Pathogenesis, Prevention, and Treatment
- PMID: 28689842
- PMCID: PMC5950727
- DOI: 10.1016/j.jaip.2017.05.001
Asthma Exacerbations: Pathogenesis, Prevention, and Treatment
Abstract
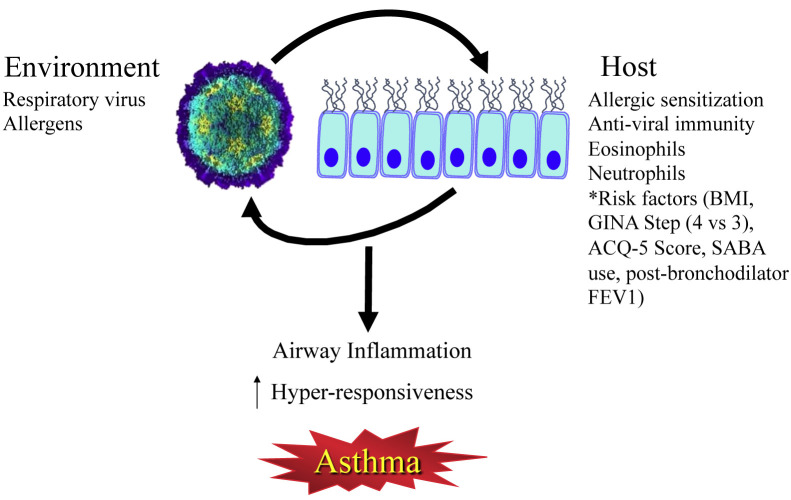
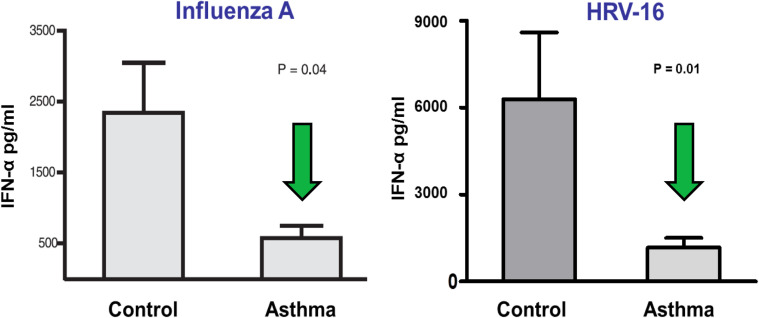
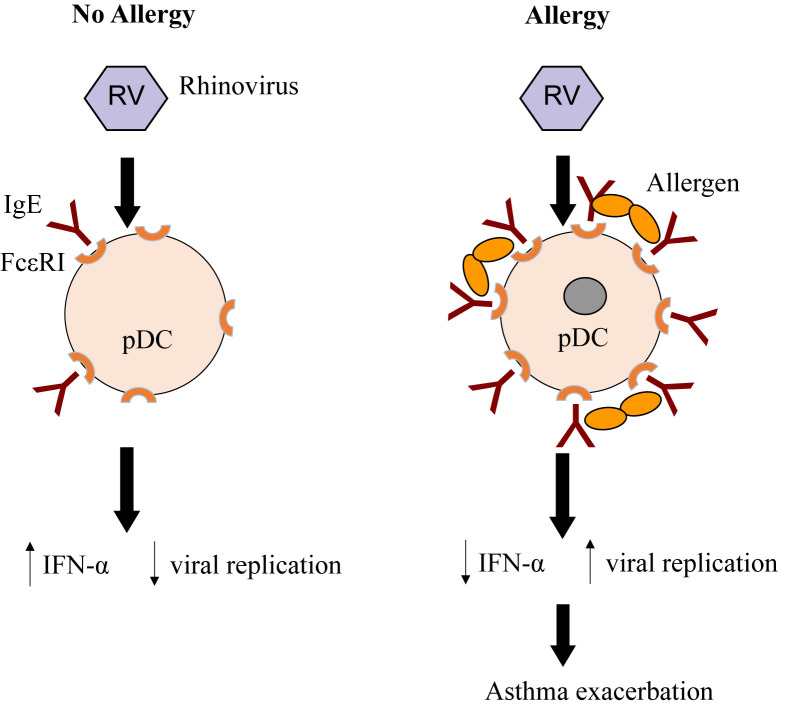
Guideline-based management of asthma focuses on disease severity and choosing the appropriate medical therapy to control symptoms and reduce the risk of exacerbations. However, irrespective of asthma severity and often despite optimal medical therapy, patients may experience acute exacerbations of symptoms and a loss of disease control. Asthma exacerbations are most commonly triggered by viral respiratory infections, particularly with human rhinovirus. Given the importance of these events to asthma morbidity and health care costs, we will review common inciting factors for asthma exacerbations and approaches to prevent and treat these events.
Keywords: Allergy; Anti-IL5; Anti-IgE; Anticholinergics; Asthma; Asthma exacerbation; Inhaled corticosteroids; Leukotriene antagonist; Long-acting β2-agonists; Prevention; Systemic corticosteroids; Treatment; Viral infection.
Copyright © 2017 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bai T.R., Vonk J.M., Postma D.S., Boezen H.M. Severe exacerbations predict excess lung function decline in asthma. Eur Respir J. 2007;30:452–456. - PubMed
-
- O'Byrne P.M., Pedersen S., Lamm C.J., Tan W.C., Busse W.W. Severe exacerbations and decline in lung function in asthma. Am J Respir Crit Care Med. 2009;179:19–24. - PubMed
-
- Ivanova J.I., Bergman R., Birnbaum H.G., Colice G.L., Silverman R.A., McLaurin K. Effect of asthma exacerbations on health care costs among asthmatic patients with moderate and severe persistent asthma. J Allergy Clin Immunol. 2012;129:1229–1235. - PubMed
-
- Barnett S.B., Nurmagambetov T.A. Costs of asthma in the United States: 2002-2007. J Allergy Clin Immunol. 2011;127:145–152. - PubMed
-
- Miller M.K., Lee J.H., Miller D.P., Wenzel S.E., Group T.S. Recent asthma exacerbations: a key predictor of future exacerbations. Respir Med. 2007;101:481–489. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
