

Hypophosphatemia after Hepatectomy or Pancreatectomy: Role of the Nicotinamide Phosphoribosyltransferase
- PMID: 28690207
- PMCID: PMC5614834
- DOI: 10.1016/j.jamcollsurg.2017.06.012
Hypophosphatemia after Hepatectomy or Pancreatectomy: Role of the Nicotinamide Phosphoribosyltransferase
Abstract
Background: Postoperative hypophosphatemia is common and is associated with a lower risk of liver failure after hepatectomy, but higher morbidity after pancreatectomy. Whether different physiologic mechanisms underlie the hypophosphatemia associated with these very different clinical outcomes is unclear. This study aims to evaluate the underlying mechanism in postoperative hypophosphatemia.
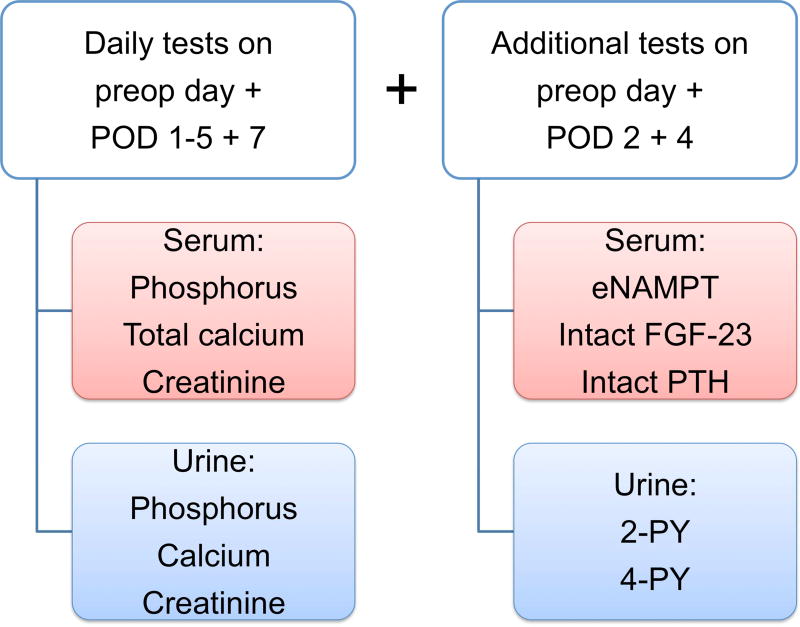
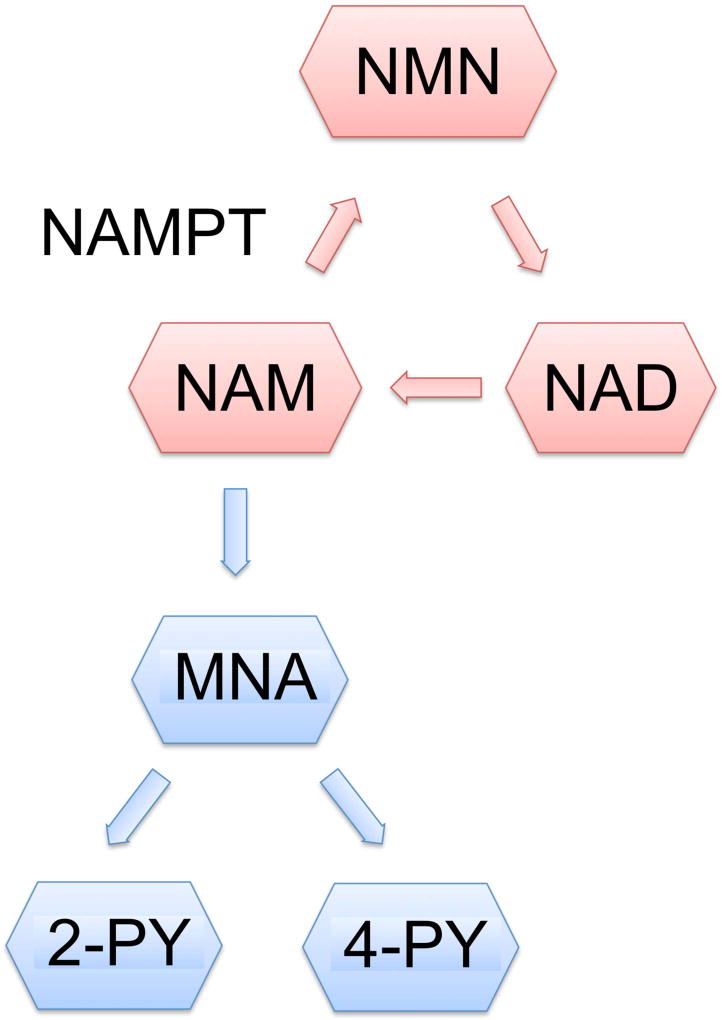
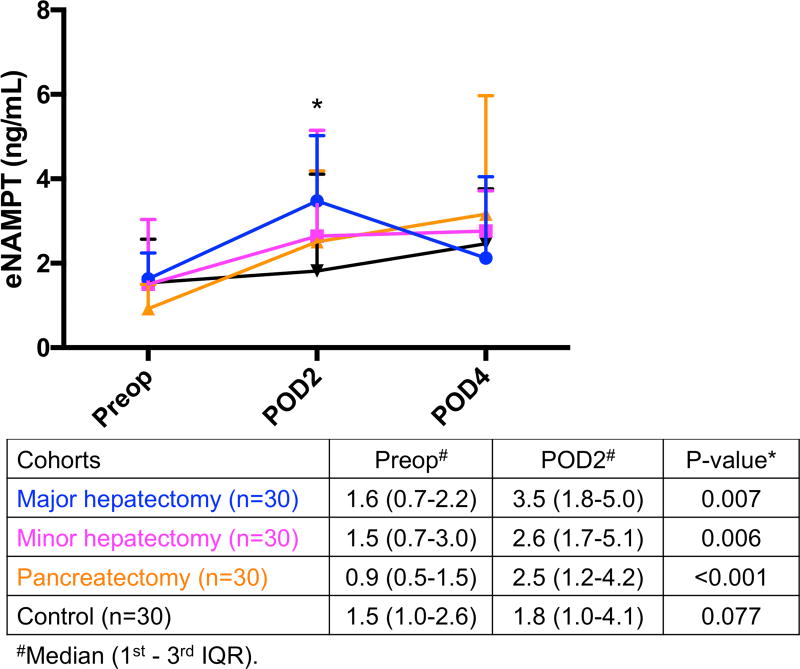
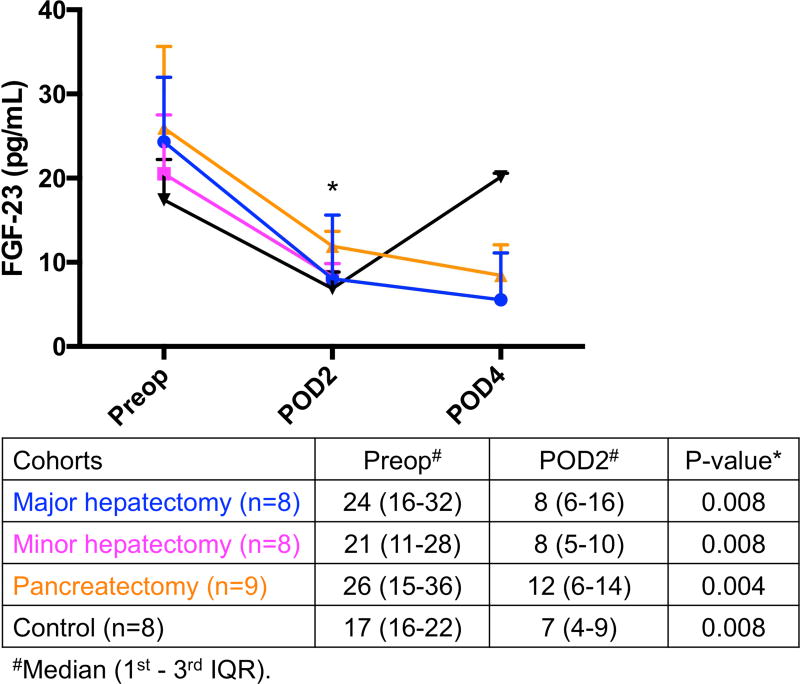
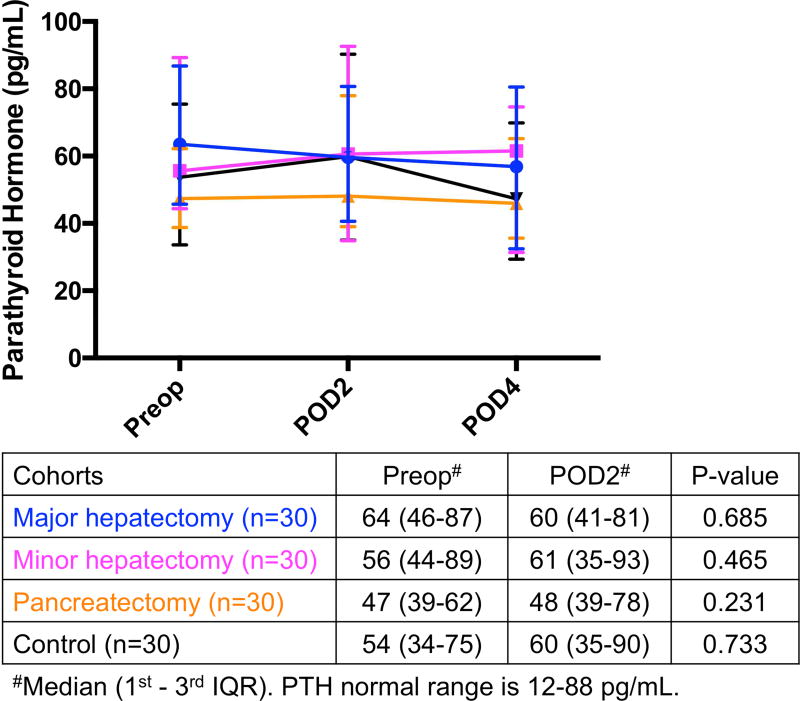
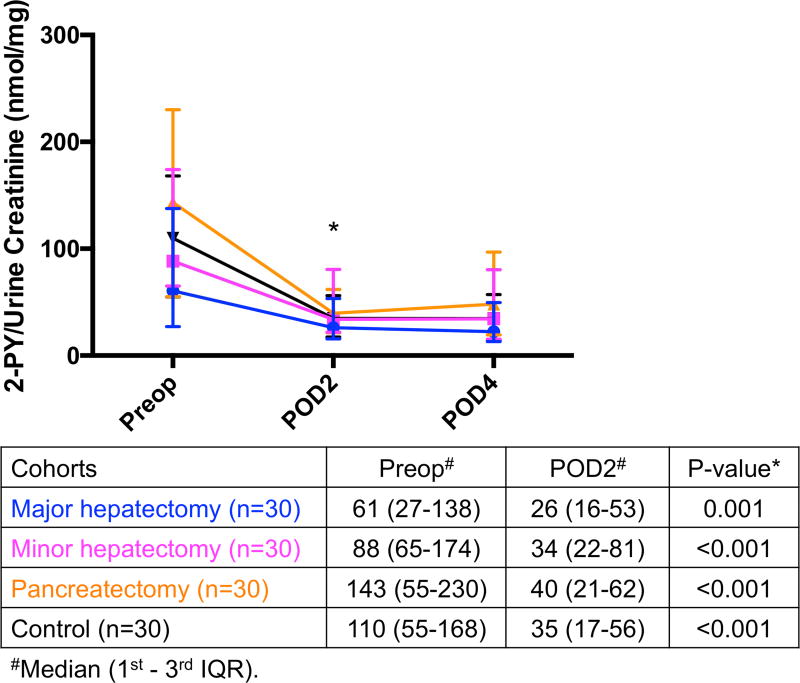
Study design: We prospectively enrolled 120 patients who underwent major hepatectomy (n = 30), minor hepatectomy (n = 30), pancreatectomy (n = 30), and laparotomy without resection (control group, n = 30). Preoperative and postoperative serum and urinary phosphorus, calcium, and creatinine, as well as phosphaturic factors, including serum nicotinamide phosphoribosyltransferase (NAMPT), fibroblast growth factor-23, and parathyroid hormone were measured. In addition, we evaluated urinary levels of nicotinamide catabolites, N-methyl-2-pyridone-5-carboxamide and N-methyl-4-pyridone-3-carboxamide.
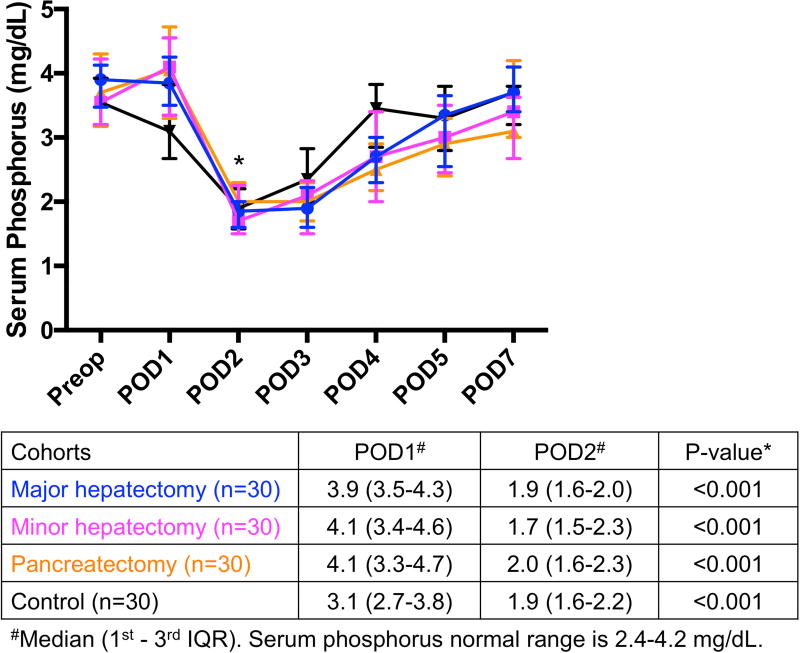
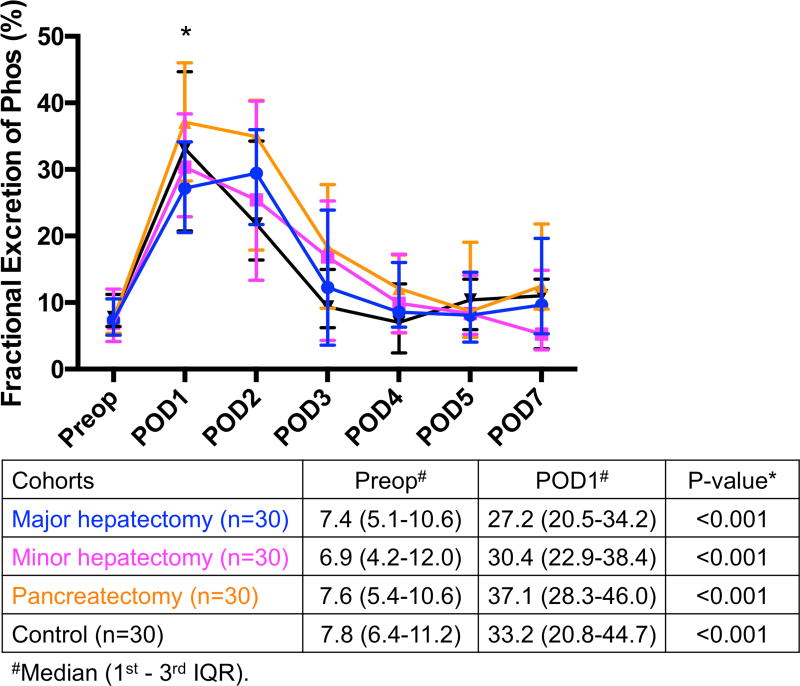
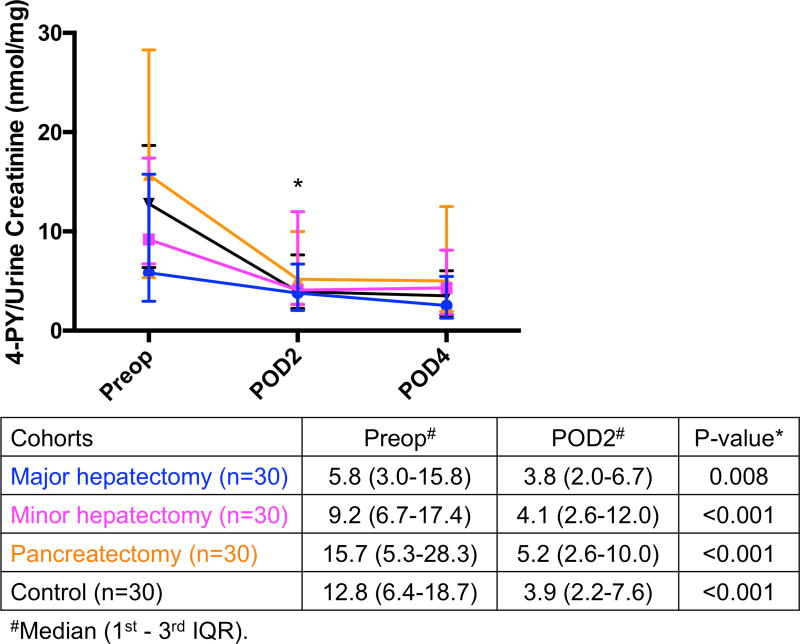
Results: We found that significant hypophosphatemia occurred from postoperative day (POD) 1 to POD 2 in all 4 groups and was preceded by hyperphosphaturia from preoperative day to POD 1. Phosphate level alterations were associated with a significant increase in NAMPT levels from preoperative day to POD 2 in all 3 resected groups, but not in the control group. The fibroblast growth factor-23 levels were significantly decreased postoperatively in all 4 groups, and parathyroid hormone levels did not change in any of the 4 groups. Urine levels of N-methyl-2-pyridone-5-carboxamide and N-methyl-4-pyridone-3-carboxamide decreased significantly in all 4 groups postoperatively.
Conclusions: This study demonstrates that the mechanism of hypophosphatemia is the same for both liver and pancreas resections. Postoperative hypophosphatemia is associated with increased NAMPT. The mechanism that upregulates NAMPT and its role on disparate clinical outcomes in postoperative patients warrant additional investigation.
Copyright © 2017 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Hepatectomy-related hypophosphatemia: a novel phosphaturic factor in the liver-kidney axis.J Am Soc Nephrol. 2014 Apr;25(4):761-72. doi: 10.1681/ASN.2013060569. Epub 2013 Nov 21. J Am Soc Nephrol. 2014. PMID: 24262791 Free PMC article.
-
Lower phosphate levels following pancreatectomy is associated with postoperative pancreatic fistula formation.HPB (Oxford). 2019 Jul;21(7):834-840. doi: 10.1016/j.hpb.2018.10.017. Epub 2018 Nov 29. HPB (Oxford). 2019. PMID: 30503649
-
Hepatic resection-related hypophosphatemia is of renal origin as manifested by isolated hyperphosphaturia.Ann Surg. 2005 Feb;241(2):343-8. doi: 10.1097/01.sla.0000152093.43468.c0. Ann Surg. 2005. PMID: 15650646 Free PMC article.
-
Safety and outcome of combined liver and pancreatic resections.Br J Surg. 2014 May;101(6):693-700. doi: 10.1002/bjs.9443. Epub 2014 Mar 25. Br J Surg. 2014. PMID: 24668308 Review.
-
NAD metabolism and the SLC34 family: evidence for a liver-kidney axis regulating inorganic phosphate.Pflugers Arch. 2019 Jan;471(1):109-122. doi: 10.1007/s00424-018-2204-2. Epub 2018 Sep 14. Pflugers Arch. 2019. PMID: 30218374 Review.
Cited by
-
Hypophosphatemia as a Predictor of Organ-Specific Complications Following Gastrointestinal Surgery: Analysis of 8034 Patients.World J Surg. 2019 Feb;43(2):385-394. doi: 10.1007/s00268-018-4726-3. World J Surg. 2019. PMID: 29955938 Free PMC article.
-
Postoperative Hypophosphatemia as a Prognostic Factor for Postoperative Pancreatic Fistula: A Systematic Review.Medicina (Kaunas). 2023 Jan 31;59(2):274. doi: 10.3390/medicina59020274. Medicina (Kaunas). 2023. PMID: 36837475 Free PMC article.
-
Hypophosphatemia as a prognostic tool for post-hepatectomy liver failure: A systematic review.World J Gastrointest Surg. 2023 Feb 27;15(2):249-257. doi: 10.4240/wjgs.v15.i2.249. World J Gastrointest Surg. 2023. PMID: 36896296 Free PMC article.
-
Efficacy and Safety of Tenapanor in Patients with Hyperphosphatemia Receiving Maintenance Hemodialysis: A Randomized Phase 3 Trial.J Am Soc Nephrol. 2019 Apr;30(4):641-652. doi: 10.1681/ASN.2018080832. Epub 2019 Mar 7. J Am Soc Nephrol. 2019. PMID: 30846557 Free PMC article. Clinical Trial.
-
Hypophosphatemia in Patients With Multiple Myeloma.Cureus. 2023 Jun 15;15(6):e40487. doi: 10.7759/cureus.40487. eCollection 2023 Jun. Cureus. 2023. PMID: 37342302 Free PMC article. Review.
References
-
- Rasmussen A, Kimose HH, Hessov I. Severity of postoperative hypophosphatemia in relation to glucose administration and renal handling of phosphate. Acta Chir Scand. 1988;154:617–621. - PubMed
-
- Cohen J, Kogan A, Sahar G, et al. Hypophosphatemia following open heart surgery: incidence and consequences. Eur J Cardiothorac Surg. 2004;26:306–310. - PubMed
-
- Datta HK, Malik M, Neely RD. Hepatic surgery-related hypophosphatemia. Clin Chim Acta. 2007;380:13–23. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
