

Breakthrough attacks in patients with hereditary angioedema receiving long-term prophylaxis are responsive to icatibant: findings from the Icatibant Outcome Survey
- PMID: 28690642
- PMCID: PMC5497380
- DOI: 10.1186/s13223-017-0203-z
Breakthrough attacks in patients with hereditary angioedema receiving long-term prophylaxis are responsive to icatibant: findings from the Icatibant Outcome Survey
Abstract
Background: Patients with hereditary angioedema (HAE) due to C1-inhibitor deficiency (C1-INH-HAE) experience recurrent attacks of cutaneous or submucosal edema that may be frequent and severe; prophylactic treatments can be prescribed to prevent attacks. However, despite the use of long-term prophylaxis (LTP), breakthrough attacks are known to occur. We used data from the Icatibant Outcome Survey (IOS) to evaluate the characteristics of breakthrough attacks and the effectiveness of icatibant as a treatment option.
Methods: Data on LTP use, attacks, and treatments were recorded. Attack characteristics, treatment characteristics, and outcomes (time to treatment, time to resolution, and duration of attack) were compared for attacks that occurred with versus without LTP.
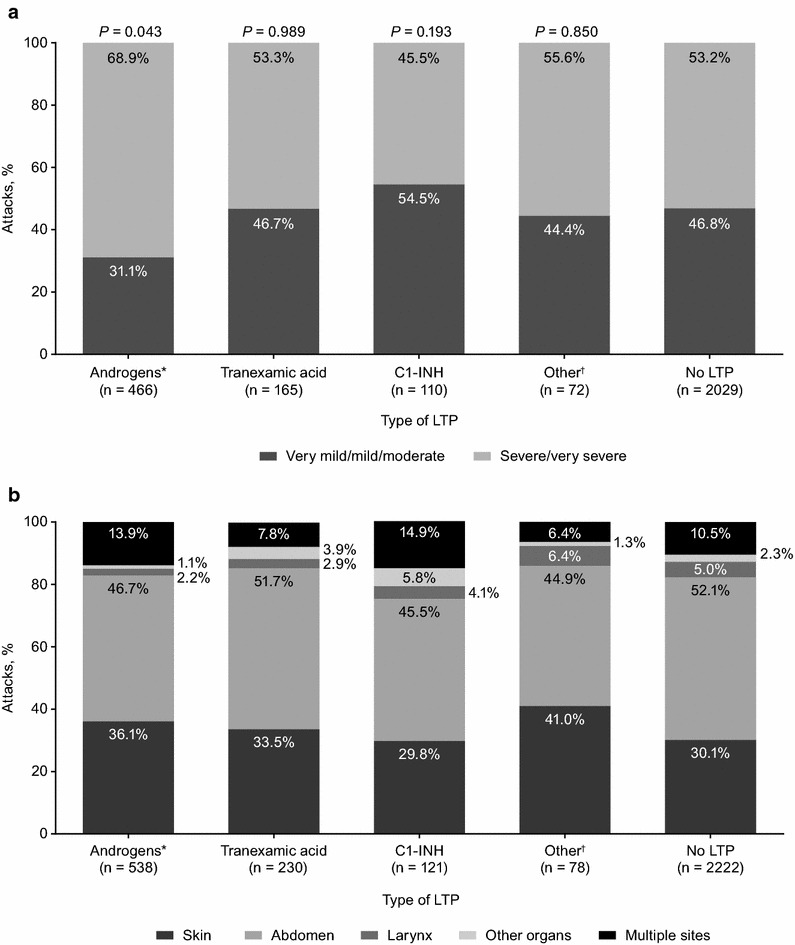
Results: Data on 3228 icatibant-treated attacks from 448 patients with C1-INH-HAE were analyzed; 30.1% of attacks occurred while patients were using LTP. Attack rate, attack severity, and the distribution of attack sites were similar across all types of LTP used, and were comparable to the results found in patients who did not receive LTP. Attacks were successfully treated with icatibant; 82.5% of all breakthrough attacks were treated with a single icatibant injection without C1-INH rescue medication. Treatment outcomes were comparable for breakthrough attacks across all LTP types, and for attacks without LTP.
Conclusions: Patients who use LTP should be aware that breakthrough attacks can occur, and such attacks can be severe. Thus, patients with C1-INH-HAE using LTP should have emergency treatment readily available. Data from IOS show that icatibant is effective for the treatment of breakthrough attacks. Trial Registration NCT01034969.
Keywords: Bradykinin; Breakthrough attacks; Hereditary angioedema; Icatibant; Prophylaxis.
Figures

References
-
- Zuraw BL, Bernstein JA, Lang DM, Craig T, Dreyfus D, Hsieh F, et al. A focused parameter update: hereditary angioedema, acquired C1 inhibitor deficiency, and angiotensin-converting enzyme inhibitor-associated angioedema. J Allergy Clin Immunol. 2013;131:1491–1493. doi: 10.1016/j.jaci.2013.03.034. - DOI - PubMed
-
- Cicardi M, Bork K, Caballero T, Craig T, Li HH, Longhurst H, et al. Evidence-based recommendations for the therapeutic management of angioedema owing to hereditary C1 inhibitor deficiency: consensus report of an International Working Group. Allergy. 2012;67:147–157. doi: 10.1111/j.1398-9995.2011.02751.x. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
