

Hepatic or Cystic Artery Pseudoaneurysms Following a Laparoscopic Cholecystectomy: Literature review of aetiopathogenesis, presentation, diagnosis and management
- PMID: 28690884
- PMCID: PMC5488813
- DOI: 10.18295/squmj.2016.17.02.002
Hepatic or Cystic Artery Pseudoaneurysms Following a Laparoscopic Cholecystectomy: Literature review of aetiopathogenesis, presentation, diagnosis and management
Abstract
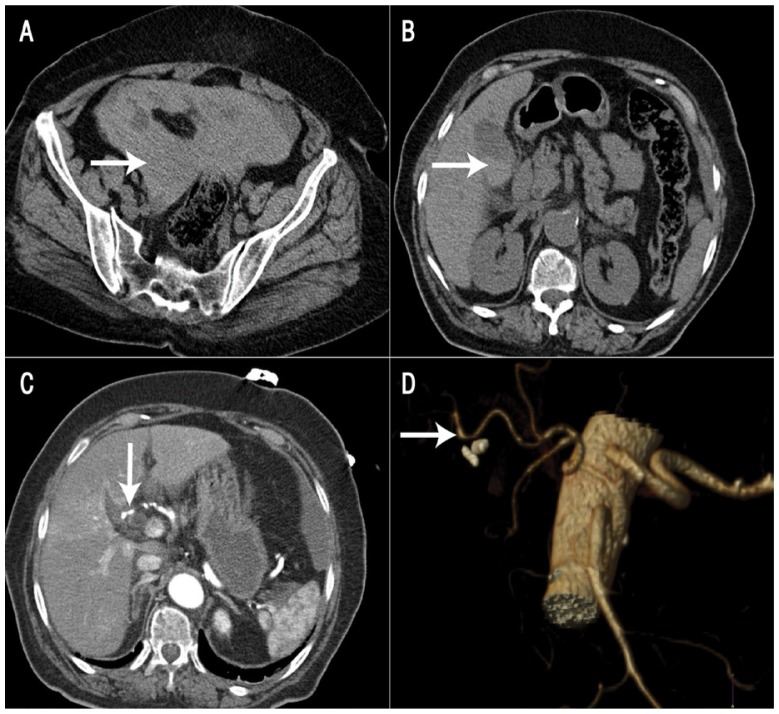
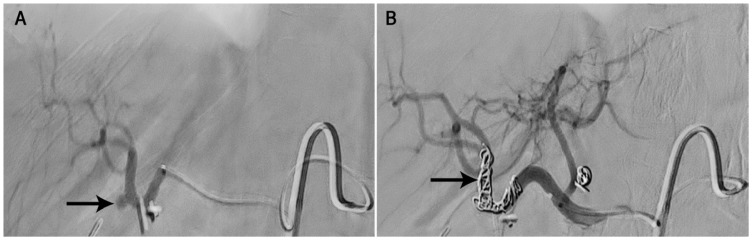
Pseudoaneurysms (PSAs) of the hepatic and/or cystic artery are a rare complication following a laparoscopic cholecystectomy (LC). Generally, PSA cases present with haemobilia several weeks following the procedure. Transarterial embolisation (TAE) is considered the optimal management approach. We report a 70-year-old woman who presented to the Sultan Qaboos University Hospital, Muscat, Oman, in 2016 with massive hemoperitoneum two weeks after undergoing a LC procedure in another hospital. She was successfully managed using coil TAE. An extensive literature review revealed 101 cases of hepatic or cystic artery PSAs following a LC procedure. Haemobilia was the main presentation (85.1%) and the mean time of postoperative presentation was 36 days. The hepatic artery was involved in most cases (88.1%), followed by the cystic artery (7.9%) and a combination of both (4.0%). Most cases were managed with TAE (72.3%), with a 94.5% success rate. The overall mortality rate was 2.0%.
Keywords: Hemoperitoneum; Hepatic Artery; Laparoscopic Cholecystectomy; Pseudoaneurysm; Therapeutic Embolization.
Figures
References
-
- Madanur MA, Battula N, Sethi H, Deshpande R, Heaton N, Rela M. Pseudoaneurysm following laparoscopic cholecystectomy. Hepatobiliary Pancreat Dis Int. 2007;6:294–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous