

Fluorescence In Situ Hybridization for Diagnosis of Whipple's Disease in Formalin-Fixed Paraffin-Embedded Tissue
- PMID: 28691008
- PMCID: PMC5479881
- DOI: 10.3389/fmed.2017.00087
Fluorescence In Situ Hybridization for Diagnosis of Whipple's Disease in Formalin-Fixed Paraffin-Embedded Tissue
Abstract
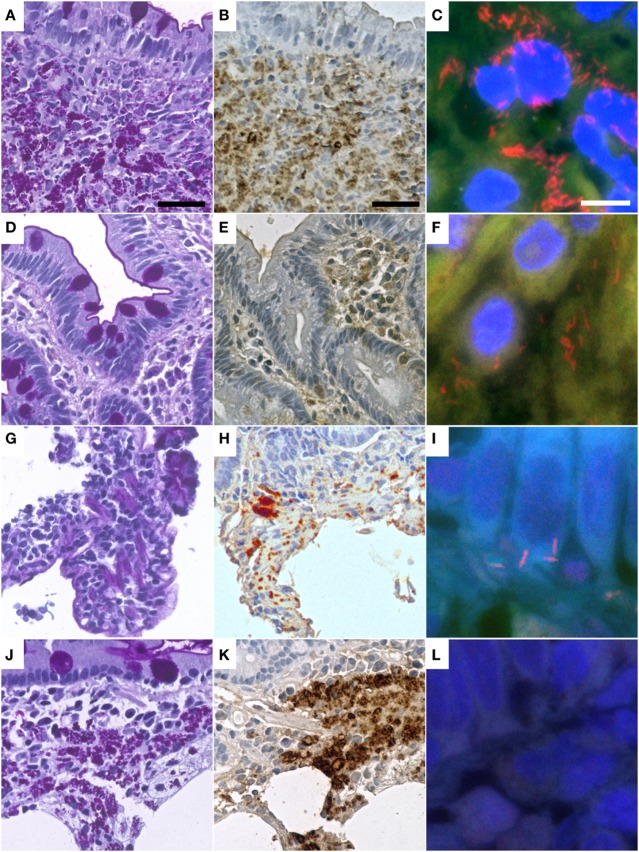
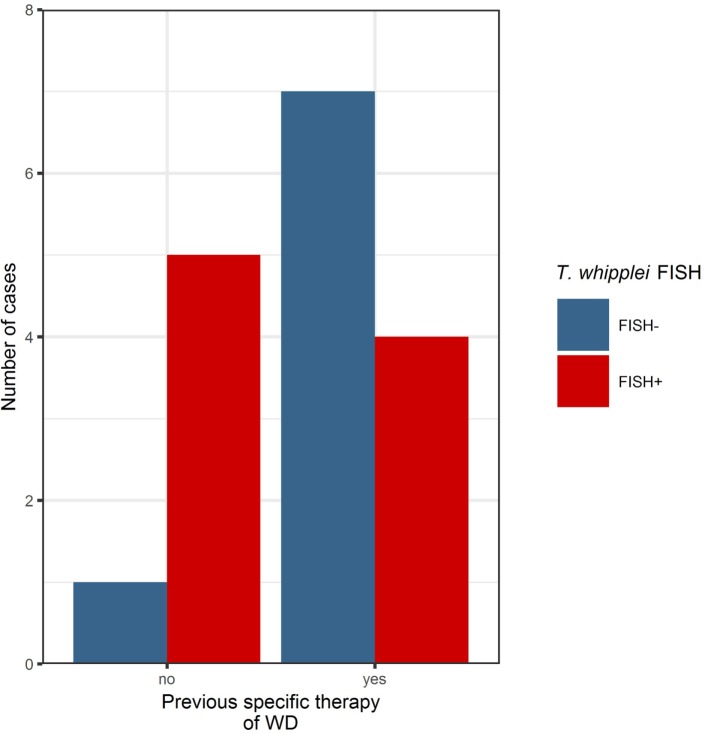
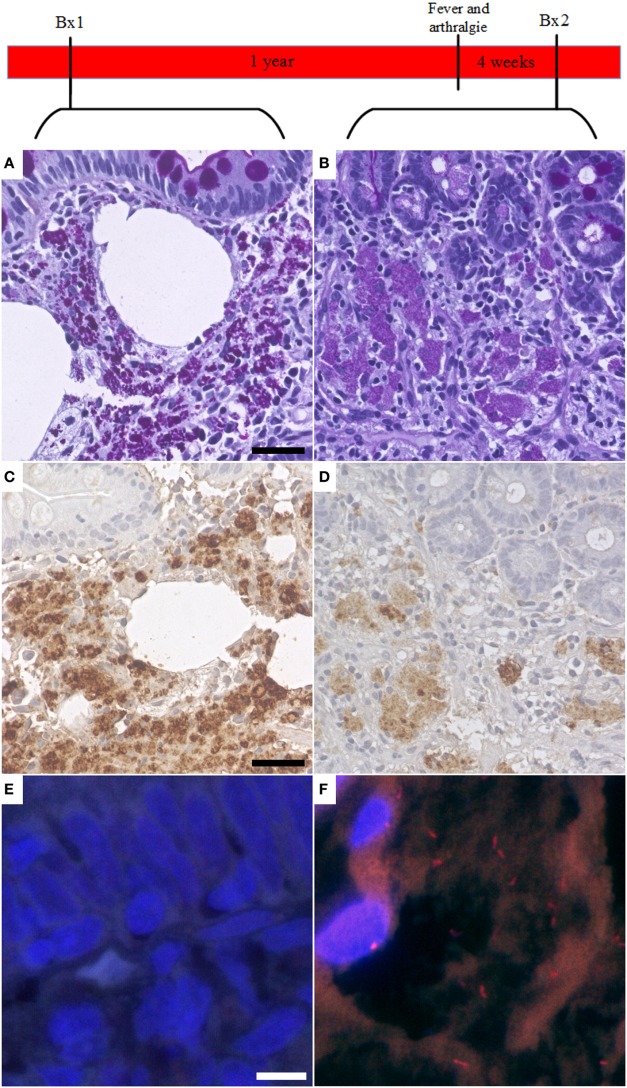
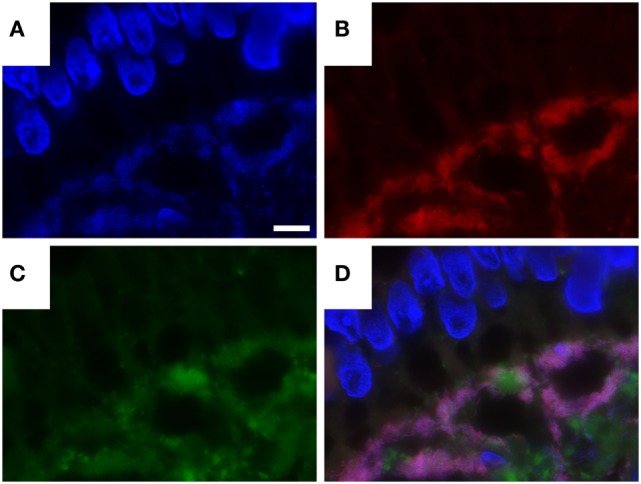
Whipple's disease (WD) is a rare chronic systemic infection with a wide range of clinical symptoms, routinely diagnosed in biopsies from the small intestine and other tissues by periodic acid-Schiff (PAS) diastase staining and immunohistological analysis with specific antibodies. The aim of our study was to improve the pathological diagnosis of WD. Therefore, we analyzed the potential of fluorescence in situ hybridization (FISH) for diagnosing WD, using a Tropheryma (T.) whipplei-specific probe. 19 formalin-fixed paraffin-embedded (FFPE) duodenal biopsy specimens of 12 patients with treated (6/12) and untreated (6/12) WD were retrospectively examined using PAS diastase staining, immunohistochemistry, and FISH. 20 biopsy specimens with normal intestinal mucosa, Helicobacter pylori, or mycobacterial infection, respectively, served as controls. We successfully detected T. whipplei in tissue biopsies with a sensitivity of 83% in untreated (5/6) and 40% in treated (4/10) cases of WD. In our study, we show that FISH-based diagnosis of individual vital T. whipplei in FFPE specimens is feasible and can be considered as ancillary diagnostic tool for the diagnosis of WD in FFPE material. We show that FISH not only detect active WD but also be helpful as an indicator for the efficiency of antibiotic treatment and for detection of recurrence of disease when the signal of PAS diastase and immunohistochemistry lags behind the recurrence of disease, especially if the clinical course of the patient and antimicrobial treatment is considered.
Keywords: Tropheryma whipplei; Whipple’s disease; fluorescence in situ hybridization; formalin-fixed paraffin-embedded tissue; immunohistochemistry.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources