

HIV viral load as an independent risk factor for tuberculosis in South Africa: collaborative analysis of cohort studies
- PMID: 28691438
- PMCID: PMC5515052
- DOI: 10.7448/IAS.20.1.21327
HIV viral load as an independent risk factor for tuberculosis in South Africa: collaborative analysis of cohort studies
Abstract
Introduction: Chronic immune activation due to ongoing HIV replication may lead to impaired immune responses against opportunistic infections such as tuberculosis (TB). We studied the role of HIV replication as a risk factor for incident TB after starting antiretroviral therapy (ART).
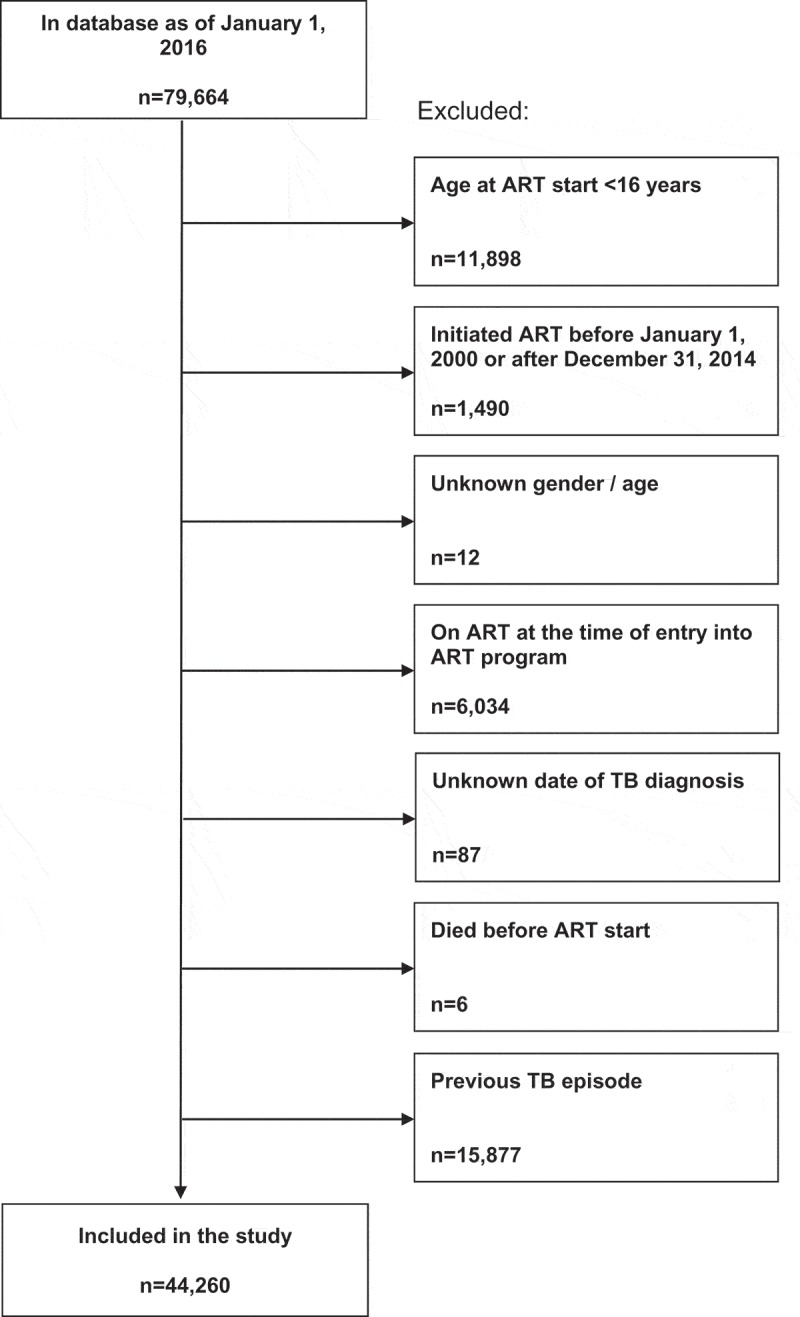
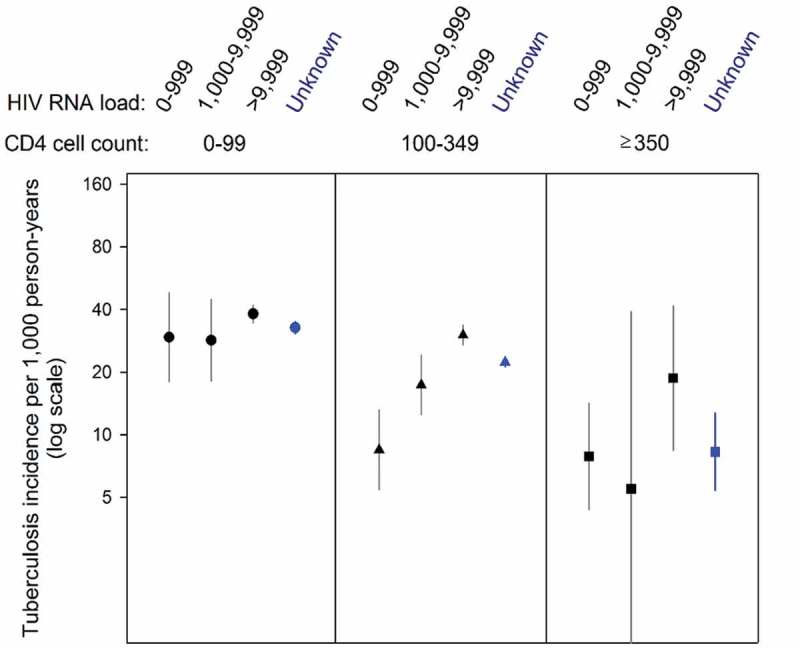
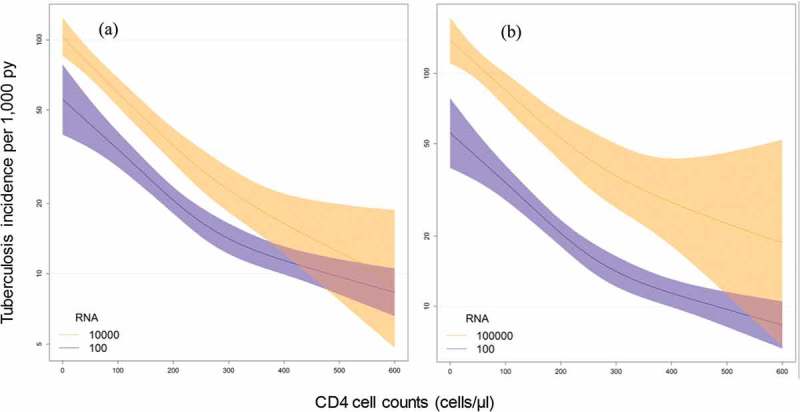
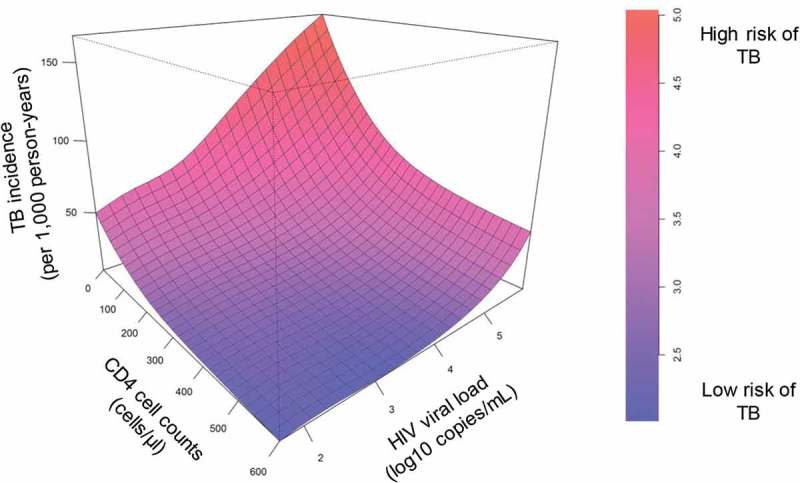
Methods: We included all HIV-positive adult patients (≥16 years) in care between 2000 and 2014 at three ART programmes in South Africa. Patients with previous TB were excluded. Missing CD4 cell counts and HIV-RNA viral loads at ART start (baseline) and during follow-up were imputed. We used parametric survival models to assess TB incidence (pulmonary and extrapulmonary) by CD4 cell and HIV-RNA levels, and estimated the rate ratios for TB by including age, sex, baseline viral loads, CD4 cell counts, and WHO clinical stage in the model. We also used Poisson general additive regression models with time-updated CD4 and HIV-RNA values, adjusting for age and sex.
Results: We included 44,260 patients with a median follow-up time of 2.7 years (interquartile range [IQR] 1.0-5.0); 3,819 incident TB cases were recorded (8.6%). At baseline, the median age was 34 years (IQR 28-41); 30,675 patients (69.3%) were female. The median CD4 cell count was 156 cells/µL (IQR 79-229) and the median HIV-RNA viral load 58,000 copies/mL (IQR 6,000-240,000). Overall TB incidence was 26.2/1,000 person-years (95% confidence interval [CI] 25.3-27.0). Compared to the lowest viral load category (0-999 copies/mL), the adjusted rate ratio for TB was 1.41 (95% CI 1.15-1.75, p < 0.001) in the highest group (>10,000 copies/mL). Time-updated analyses for CD4/HIV-RNA confirmed the association of viral load with the risk for TB.
Conclusions: Our results indicate that ongoing HIV replication is an important risk factor for TB, regardless of CD4 cell counts, and underline the importance of early ART start and retention on ART.
Keywords: CD4 cell count; HIV; antiretroviral treatment; incidence; opportunistic infection; prediction; time-updated; tuberculosis; viral load.
Figures
References
-
- World Health Organization Global tuberculosis report 2014. World Health Organization Document. 2014;WHO/HTM/TB/2014.08:1–7.
-
- Moore RD, Chaisson RE.. Natural history of opportunistic disease in an HIV-infected urban clinical cohort. Ann Intern Med. 1996;124(7):633–42. - PubMed
-
- Corbett EL, Churchyard GJ, Charalambos S, Samb B, Moloi V, Clayton TC, et al. Morbidity and mortality in South African gold miners: impact of untreated disease due to human immunodeficiency virus. Clin Infect Dis. 2002;34(9):1251–58. - PubMed
-
- Holmes CB, Losina E, Walensky RP, Yazdanpanah Y, Freedberg KA. Review of human immunodeficiency virus type 1-related opportunistic infections in sub-Saharan Africa. Clin Infect Dis. 2003;36(5):652–62. - PubMed
-
- Ledergerber B, Egger M, Opravil M, Telenti A, Hirschel B, Battegay M, et al. Clinical progression and virological failure on highly active antiretroviral therapy in HIV-1 patients: a prospective cohort study. Swiss HIV Cohort Study. Lancet. 1999;353(9156):863–68. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
