

High risk of loss to follow-up among South African children on ART during transfer, a retrospective cohort analysis with community tracing
- PMID: 28691440
- PMCID: PMC5515030
- DOI: 10.7448/IAS.20.1.21748
High risk of loss to follow-up among South African children on ART during transfer, a retrospective cohort analysis with community tracing
Abstract
Introduction: Decentralization of HIV care for children has been recommended to improve paediatric outcomes by making antiretroviral treatment (ART) more accessible. We documented outcomes of children transferred after initiating ART at a large tertiary hospital in the Eastern Cape of South Africa.
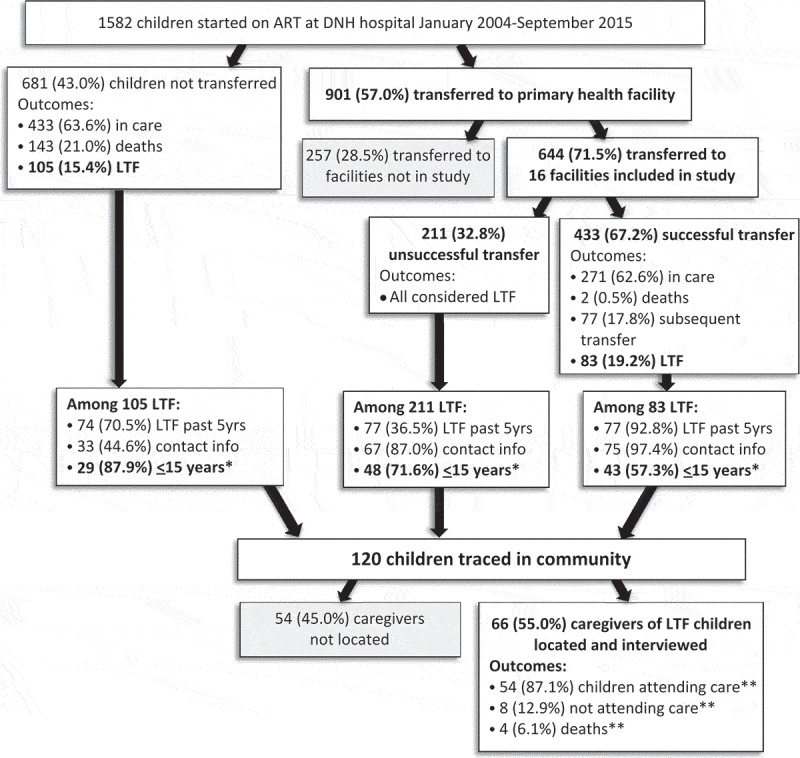
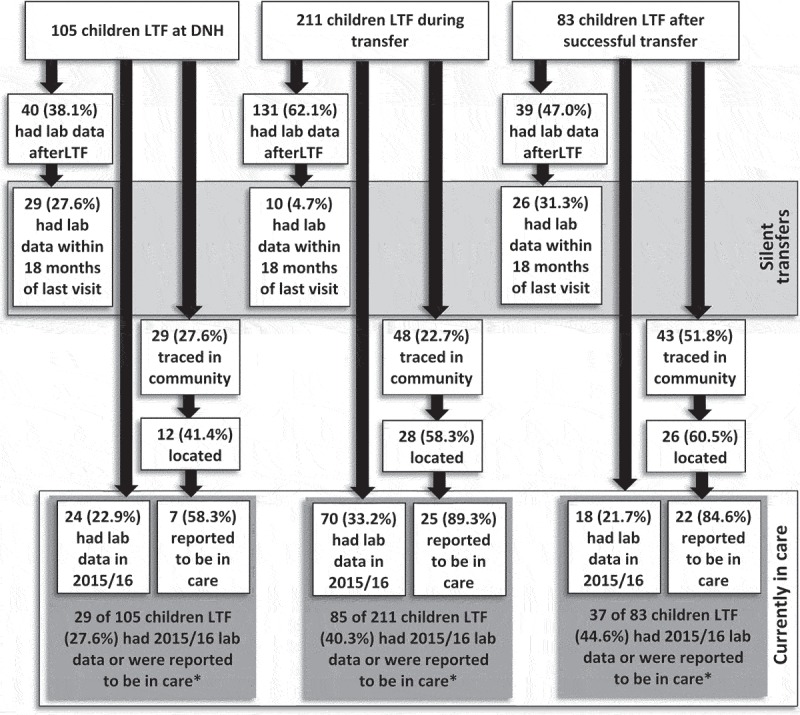
Methods: Electronic medical records for all children 0-15 years initiating ART at Dora Nginza Hospital (DNH) in Port Elizabeth, South Africa January 2004 to September 2015 were examined. Records for children transferred to primary and community clinics were searched at 16 health facilities to identify children with successful (at least one recorded visit) and unsuccessful transfer (no visits). We identified all children lost to follow-up (LTF) after ART initiation: those LTF at DNH (no visit >6 months), children with unsuccessful transfer, and children LTF after successful transfer (no visit >6 months). Community tracing was conducted to locate caregivers of children LTF and electronic laboratory data were searched to measure reengagement in care, including silent transfers.
Results: 1,582 children initiated ART at median age of 4 years [interquartile range (IQR): 1-8] and median CD4+ of 278 cells/mm3 [IQR: 119-526]. A total of 901 (57.0%) children were transferred, 644 (71.5%) to study facilities; 433 (67.2%) children had successful transfer and 211 (32.8%) had unsuccessful transfer. In total, 399 children were LTF: 105 (26.3%) from DNH, 211 (52.9%) through unsuccessful transfer and 83 (20.8%) following successful transfer. Community tracing was conducted for 120 (30.1%) of 399 children LTF and 66 (55.0%) caregivers were located and interviewed. Four children had died. Among 62 children still alive, 8 (12.9%) were reported to not be in care or taking ART and 18 (29.0%) were also not taking ART. Overall, 65 (16.3%) of 399 children LTF had a laboratory result within 18 months of their last visit indicating silent transfer and 112 (28.1%) had lab results from 2015 to 2016 indicating current care.
Conclusion: We found that only two-thirds of children on ART transferred to primary and community health clinics had successful transfer. These findings suggest that transfer is a particularly vulnerable step in the paediatric HIV care cascade.
Keywords: ART; decentralization; loss to follow-up; paediatric HIV; referral; retention.
Conflict of interest statement
None of the authors have competing interests to declare.
Figures
References
-
- UNAIDS Children and HIV: fact Sheet. Geneva: UNAIDS; 2016.
-
- Kline MW, Ferris MG, Jones DC, Calles NR, Mizwa MB, Schwarzwald HL, et al. The pediatric AIDS corps: responding to the African HIV/AIDS health professional resource crisis. Pediatrics. 2009;123(1):134–11. - PubMed
-
- Waning B, Diedrichsen E, Jambert E, Barnighausen T, Li Y, Pouw M, et al. The global pediatric antiretroviral market: analyses of product availability and utilization reveal challenges for development of pediatric formulations and HIV/AIDS treatment in children. BMC Pediatr. 2010;10:74. - PMC - PubMed
-
- Penazzato M, Davies MA, Apollo T, Negussie E, Ford N. Task shifting for the delivery of pediatric antiretroviral treatment: a systematic review. J Acquire Immune Defic Syndr. 2014;75(4):414–22. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
