

Investigational antiarrhythmic agents: promising drugs in early clinical development
- PMID: 28691539
- PMCID: PMC6324729
- DOI: 10.1080/13543784.2017.1353601
Investigational antiarrhythmic agents: promising drugs in early clinical development
Abstract
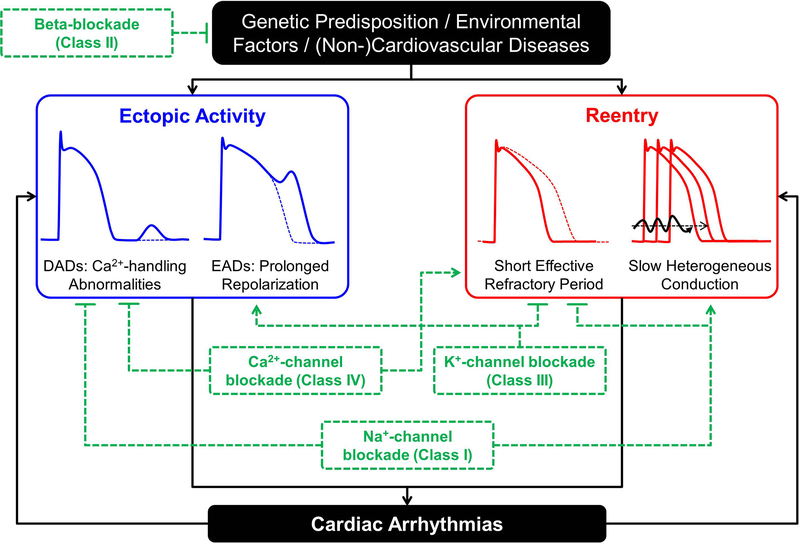
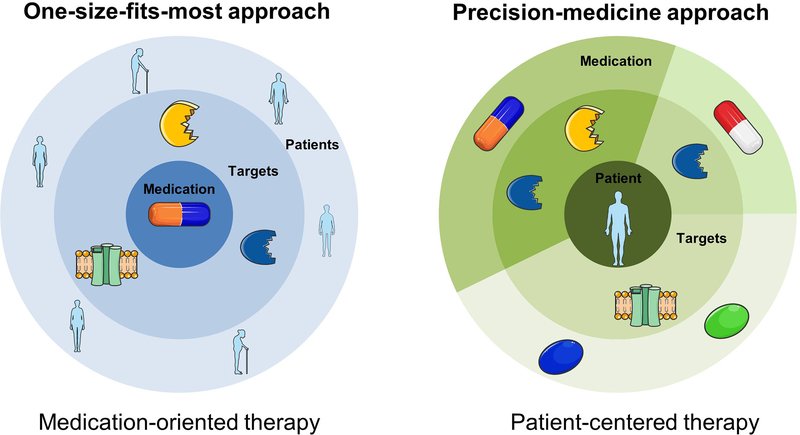
Although there have been important technological advances for the treatment of cardiac arrhythmias (e.g., catheter ablation technology), antiarrhythmic drugs (AADs) remain the cornerstone therapy for the majority of patients with arrhythmias. Most of the currently available AADs were coincidental findings and did not result from a systematic development process based on known arrhythmogenic mechanisms and specific targets. During the last 20 years, our understanding of cardiac electrophysiology and fundamental arrhythmia mechanisms has increased significantly, resulting in the identification of new potential targets for mechanism-based antiarrhythmic therapy. Areas covered: Here, we review the state-of-the-art in arrhythmogenic mechanisms and AAD therapy. Thereafter, we focus on a number of antiarrhythmic targets that have received significant attention recently: atrial-specific K+-channels, the late Na+-current, the cardiac ryanodine-receptor channel type-2, and the small-conductance Ca2+-activated K+-channel. We highlight for each of these targets available antiarrhythmic agents and the evidence for their antiarrhythmic effect in animal models and early clinical development. Expert opinion: Targeting AADs to specific subgroups of well-phenotyped patients is likely necessary to detect improved outcomes that may be obscured in the population at large. In addition, specific combinations of selective AADs may have synergistic effects and may enable a mechanism-based tailored antiarrhythmic therapy.
Keywords: Antiarrhythmic drugs; atrial fibrillation; calcium handling; ion channels; sudden cardiac death.
Conflict of interest statement
Declaration of Interest
D. Dobrev is on the Scientific Advisory Board of OMEICOS and received speaker’s fees from Boston Scientific, Daiichi Sankyo and Servier. His laboratory executed a research contract for Omeicos. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
- Priori SG, Blomstrom-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36:2793–867. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–962. - PubMed
-
- Arrhythmias Kjekshus J. and mortality in congestive heart failure. Am J Cardiol. 1990;65:42I–8I. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous