

Gastric paraganglioma: case report and review of the literature
- PMID: 28691673
- PMCID: PMC5509390
- DOI: 10.11138/gchir/2017.38.2.084
Gastric paraganglioma: case report and review of the literature
Abstract
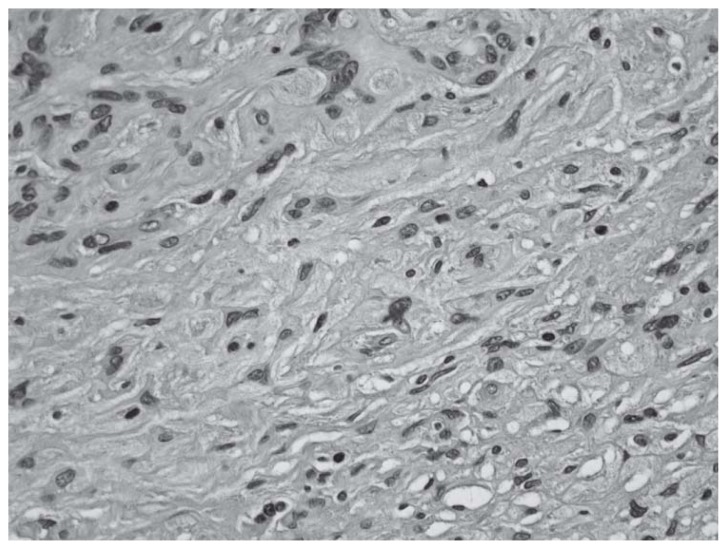
Very few cases of gastric paragangliomas have been reported in the literature to date. We report a rare case of parietal gastric paraganglioma fortuitously detected during intraoperative exploration. A 82-years-old woman presented to our emergency room for abdominal pain. On physical examination abdomen was painful on palpation and Blumberg's sign was present. The laboratory exams showed a neutrophilia in absence of leukocytosis. Acute appendicitis was suspected and a laparoscopy was performed. At exploration, the vermiform appendix was normal while a lumpy, hard-fibrous and white-pinkish extraluminal lesion of the anterior wall of the gastric body near the greater curvature of about 2 cm in diameter was present. Laparoscopic resection of the gastric lesion was performed. The patient was discharged in good condition in the fourth postoperative day. Pathologic examination revealed a gangliocitic paraganglioma. The patient is alive and well without evidence of relapse 6 months after surgery. Gastric paraganglioma is a very rare tumor and its diagnosis is very difficult. Surgical excision is the treatment of choice which can be performed successfully with laparoscopy.
Figures




References
-
- Calò PG, Lai ML, Guaitoli E, Pisano G, Favoriti P, Nicolosi A, Pinna G, Sorrenti S. Difficulties in the Diagnosis of Thyroid Paraganglioma: a Clinical Case. Clin Ter. 2013;164:e35–9. - PubMed
-
- Laforga JB, Vaquero M, Juanpere N. Paragastric Paraganglioma: A case Report With Unusual Alveolar Pattern and Myxoid Component. Diagn Cytopathol. 2012;40:815–9. - PubMed
-
- Pruiti V, Mazzeo F, Rossitto M, Foti A, Macrì A, Cucinotta E. Gastric paraganglioma: A case report and a review of the literature. Ann Ital Chir. 2014 Dec;29:85. (ePub). pii: S2239253X14023469. - PubMed
-
- Crosbie J, Humphreys WG, Maxwell M, Maxwell P, Cameron CHS, Toner PG. Gastric paraganglioma: an immunohistological and ultrastructural case study. J Submicrosc Cytol Pathol. 1990;22:401–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical