

Electrocardiograms in Low-Risk Patients Undergoing an Annual Health Examination
- PMID: 28692719
- PMCID: PMC5710571
- DOI: 10.1001/jamainternmed.2017.2649
Electrocardiograms in Low-Risk Patients Undergoing an Annual Health Examination
Abstract
Importance: Clinical guidelines advise against routine electrocardiograms (ECG) in low-risk, asymptomatic patients, but the frequency and impact of such ECGs are unknown.
Objective: To assess the frequency of ECGs following an annual health examination (AHE) with a primary care physician among patients with no known cardiac conditions or risk factors, to explore factors predictive of receiving an ECG in this clinical scenario, and to compare downstream cardiac testing and clinical outcomes in low-risk patients who did and did not receive an ECG after their AHE.
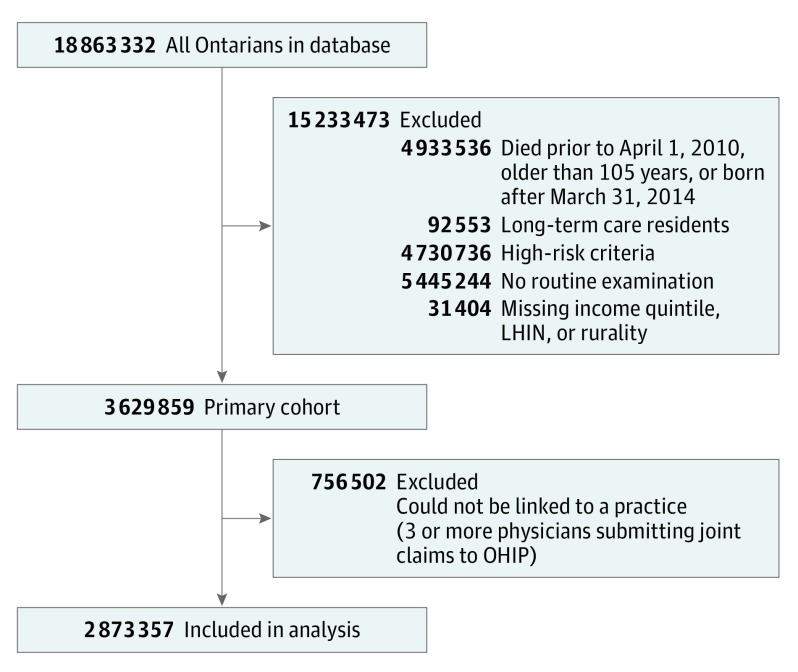
Design, setting, and participants: A population-based retrospective cohort study using administrative health care databases from Ontario, Canada, between 2010/2011 and 2014/2015 to identify low-risk primary care patients and to assess the subsequent outcomes of interest in this time frame. All patients 18 years or older who had no prior cardiac medical history or risk factors who received an AHE.
Exposures: Receipt of an ECG within 30 days of an AHE.
Main outcomes and measures: Primary outcome was receipt of downstream cardiac testing or consultation with a cardiologist. Secondary outcomes were death, hospitalization, and revascularization at 12 months.
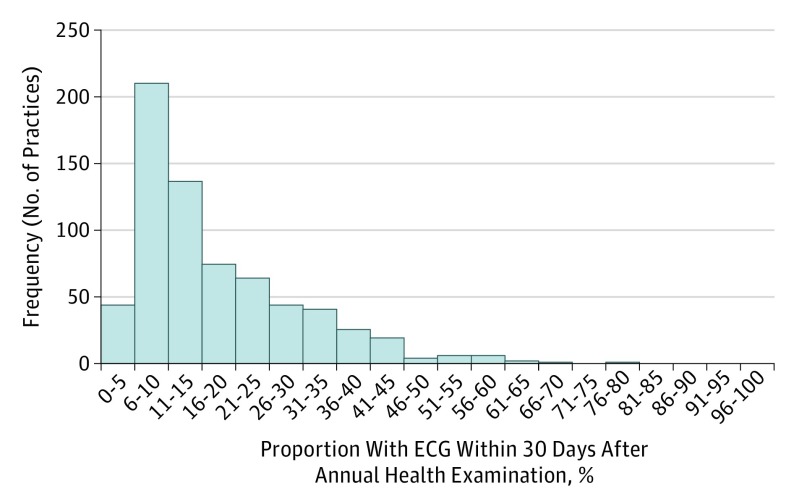
Results: A total of 3 629 859 adult patients had at least 1 AHE between fiscal years 2010/2011 and 2014/2015. Of these patients, 21.5% had an ECG within 30 days after an AHE. The proportion of patients receiving an ECG after an AHE varied from 1.8% to 76.1% among 679 primary care practices (coefficient of quartile dispersion [CQD], 0.50) and from 1.1% to 94.9% among 8036 primary care physicians (CQD, 0.54). Patients who had an ECG were significantly more likely to receive additional cardiac tests, visits, or procedures than those who did not (odds ratio [OR], 5.14; 95% CI, 5.07-5.21; P < .001). The rates of death (0.19% vs 0.16%), cardiac-related hospitalizations (0.46% vs 0.12%), and coronary revascularizations (0.20% vs 0.04%) were low in both the ECG and non-ECG cohorts.
Conclusions and relevance: Despite recommendations to the contrary, ECG testing after an AHE is relatively common, with significant variation among primary care physicians. Routine ECG testing seems to increase risk for a subsequent cardiology testing and consultation cascade, even though the overall cardiac event rate in both groups was very low.
Conflict of interest statement
Figures
Comment in
-
Screening ECGs in low-risk patients are associated with increased risk of downstream cardiac testing.BMJ Evid Based Med. 2018 Aug;23(4):150-151. doi: 10.1136/bmjebm-2018-110943. Epub 2018 Apr 19. BMJ Evid Based Med. 2018. PMID: 29674521 No abstract available.
References
-
- Institute of Medicine Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. - PubMed
-
- Wennberg JE, Fisher ES, Skinner JS. Geography and the debate over Medicare reform. Health Aff (Millwood). 2002;(suppl web exclusives):W96-114. - PubMed
-
- Levinson W, Kallewaard M, Bhatia RS, Wolfson D, Shortt S, Kerr EA; Choosing Wisely International Working Group . ‘Choosing Wisely’: a growing international campaign. BMJ Qual Saf. 2015;24(2):167-174. - PubMed
-
- Chou R, Arora B, Dana T, Fu R, Walker M, Humphrey L. Screening asymptomatic adults with resting or exercise electrocardiography: a review of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155(6):375-385. - PubMed
-
- Wolfson D, Santa J, Slass L. Engaging physicians and consumers in conversations about treatment overuse and waste: a short history of the choosing wisely campaign. Acad Med. 2014;89(7):990-995. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
