

Effects of radiofrequency ablation versus other ablating techniques on hepatocellular carcinomas: a systematic review and meta-analysis
- PMID: 28693505
- PMCID: PMC5504820
- DOI: 10.1186/s12957-017-1196-2
Effects of radiofrequency ablation versus other ablating techniques on hepatocellular carcinomas: a systematic review and meta-analysis
Abstract
Background: Percutaneous ablation has quickly arisen as one of the important alternative treatments for hepatocellular carcinoma (HCC). We aimed to compare the therapeutic effects of radiofrequency ablation (RFA) and other ablative techniques on HCCs.
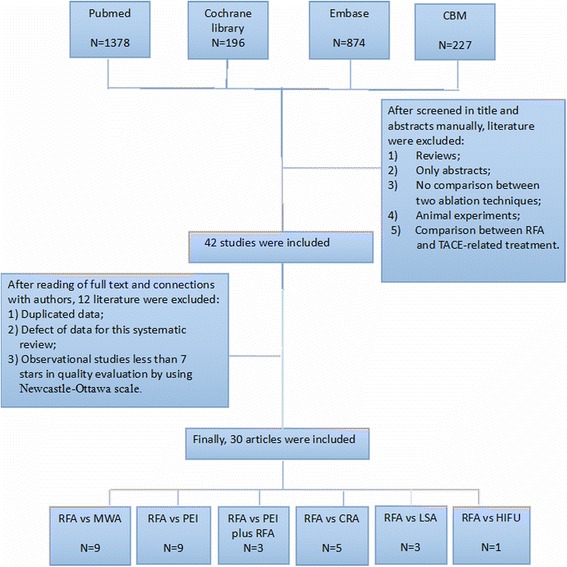
Methods: Databases were searched to identify literature on complete tumor ablation (CTA), overall survival (OS), local tumor recurrence (LTR), and complications of RFA in the treatment of HCC, compared with those of microwave ablation (MWA), percutaneous ethanol injection (PEI), PEI plus RFA, cryoablation (CRA), laser ablation (LSA), and high-intensity focused ultrasound. Randomized controlled trials and high-quality cohort studies were included in the assessment.
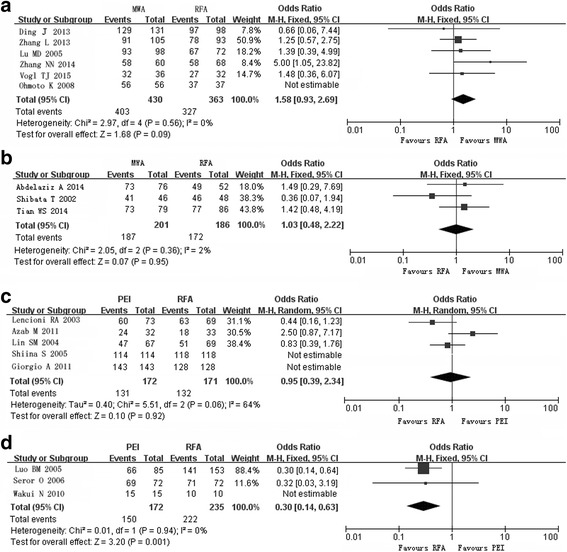
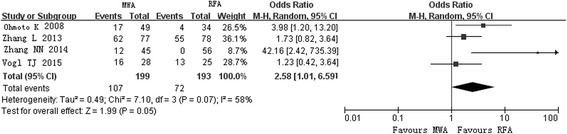
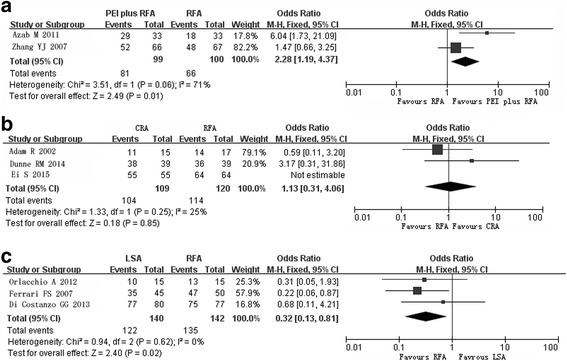
Results: The effects of MWA and CRA appeared to be similar to those of RFA, but lower rates of LTR and higher rates of CTA in large tumors compared with RFA were reported (P < 0.05). CTA rates were lower in patients treated with PEI (odds ratio [OR] 0.16, 95% confidence interval [CI] 0.06-0.42), and higher in those treated with PEI plus RFA (OR 2.28, 95% CI 1.19-3.60), with an increased incidence of fever (P < 0.05). LSA resulted in lower CTA rates (OR 0.32, 95% CI 0.13-0.81) and OS (hazard ratio 1.47, 95% CI 1.01-2.15), with a lower incidence of complications.
Conclusions: Compared with RFA, identical effects were found in MWA and CRA groups. Fewer complications were observed in PEI and LSA group. PEI plus RFA appeared more effective, with a higher rate of complications. Well-designed randomized controlled trials are further needed to confirm above results.
Keywords: Ablative techniques; Hepatocellular carcinoma; Radiofrequency ablation; Therapeutic effects.
Conflict of interest statement
Ethics approval and consent to participate
No applicable.
Consent for publication
The written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
