

Mobility of US Rural Primary Care Physicians During 2000-2014
- PMID: 28694267
- PMCID: PMC5505450
- DOI: 10.1370/afm.2096
Mobility of US Rural Primary Care Physicians During 2000-2014
Abstract
Purpose: Despite considerable investment in increasing the number of primary care physicians in rural shortage areas, little is known about their movement rates and factors influencing their mobility. We aimed to characterize geographic mobility among rural primary care physicians, and to identify location and individual factors that influence such mobility.
Methods: Using data from the American Medical Association Physician Masterfile for each clinically active US physician, we created seven 2-year (biennial) mobility periods during 2000-2014. These periods were merged with county-level "rurality," physician supply, economic characteristics, key demographic measures, and individual physician characteristics. We computed (1) mobility rates of physicians by rurality; (2) linear regression models of county-level rural nonretention (departure); and (3) logit models of physicians leaving rural practice.
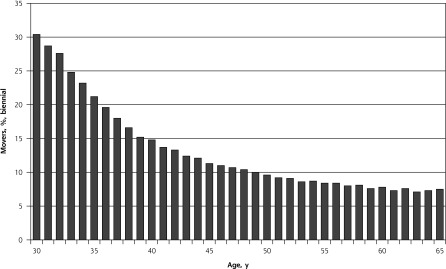
Results: Biennial turnover was about 17% among physicians aged 45 and younger, compared with 9% among physicians aged 46 to 65, with little difference between rural and metropolitan groups. County-level physician mobility was higher for counties that lacked a hospital (absolute increase = 5.7%), had a smaller population size, and had lower primary care physician supply, but area-level economic and demographic factors had little impact. Female physicians (odds ratios = 1.24 and 1.46 for those aged 45 or younger and those aged 46 to 65, respectively) and physicians born in a metropolitan area (odds ratios = 1.75 and 1.56 for those aged 45 or younger and those aged 46 to 65, respectively) were more likely to leave rural practice.
Conclusions: These flndings provide national-level evidence of rural physician mobility rates and factors associated with both county-level retention and individual-level departures. Outcomes were notably poorer in the most remote locations and those already having poorer physician supply and professional support. Rural health workforce planners and policymakers must be cognizant of these key factors to more effectively target retention policies and to take into account the additional support needed by these more vulnerable communities.
Keywords: mobility; primary care physicians; retention; rural; workforce.
© 2017 Annals of Family Medicine, Inc.
Conflict of interest statement
Conflicts of interest: authors report none.
Figures
References
-
- Ricketts TC. The migration of physicians and the local supply of practitioners: a flve-year comparison. Acad Med. 2013;88(12): 1913–1918. - PubMed
-
- Jones C, Parker T, Ahearn M, Mishra A, Variyam J. Health Status and Health Care Access of Farm and Rural Populations. Washington, DC: United States Department of Agriculture, Economic Research Service; 2009. Economic Information Bulletin Number 57.
-
- World Health Organization. Increasing Access to Health Workers in Remote and Rural Locations Through Improved Retention: Global Policy Recommendations. Geneva, Switzerland: WHO Press; 2010. - PubMed
-
- Weinhold I, Gurtner S. Understanding shortages of sufflcient health care in rural areas. Health Policy. 2014;118(2):201–214. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical