

Proposed Clinical Decision Rules to Diagnose Acute Rhinosinusitis Among Adults in Primary Care
- PMID: 28694271
- PMCID: PMC5505454
- DOI: 10.1370/afm.2060
Proposed Clinical Decision Rules to Diagnose Acute Rhinosinusitis Among Adults in Primary Care
Abstract
Purpose: To reduce inappropriate antibiotic prescribing, we sought to develop a clinical decision rule for the diagnosis of acute rhinosinusitis and acute bacterial rhinosinusitis.
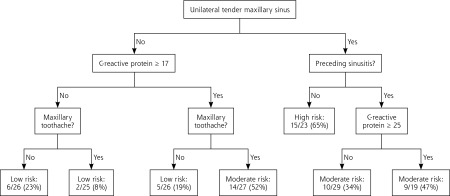
Methods: Multivariate analysis and classification and regression tree (CART) analysis were used to develop clinical decision rules for the diagnosis of acute rhinosinusitis, defined using 3 different reference standards (purulent antral puncture fluid or abnormal finding on a computed tomographic (CT) scan; for acute bacterial rhinosinusitis, we used a positive bacterial culture of antral fluid). Signs, symptoms, C-reactive protein (CRP), and reference standard tests were prospectively recorded in 175 Danish patients aged 18 to 65 years seeking care for suspected acute rhinosinusitis. For each reference standard, we developed 2 clinical decision rules: a point score based on a logistic regression model and an algorithm based on a CART model. We identified low-, moderate-, and high-risk groups for acute rhinosinusitis or acute bacterial rhinosinusitis for each clinical decision rule.
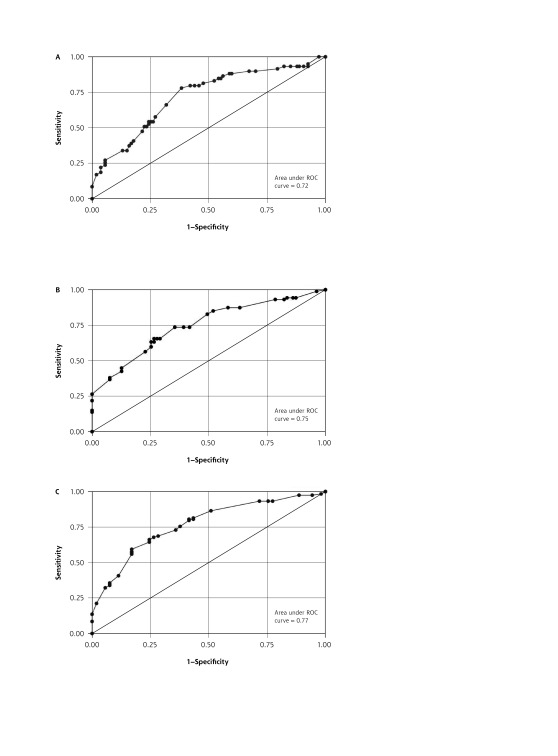
Results: The point scores each had between 5 and 6 predictors, and an area under the receiver operating characteristic curve (AUROCC) between 0.721 and 0.767. For positive bacterial culture as the reference standard, low-, moderate-, and high-risk groups had a 16%, 49%, and 73% likelihood of acute bacterial rhinosinusitis, respectively. CART models had an AUROCC ranging from 0.783 to 0.827. For positive bacterial culture as the reference standard, low-, moderate-, and high-risk groups had a likelihood of acute bacterial rhinosinusitis of 6%, 31%, and 59% respectively.
Conclusions: We have developed a series of clinical decision rules integrating signs, symptoms, and CRP to diagnose acute rhinosinusitis and acute bacterial rhinosinusitis with good accuracy. They now require prospective validation and an assessment of their effect on clinical and process outcomes.
Keywords: clinical decision making; clinical decision rule; point score; primary care; respiratory tract infections; rhinosinusitis; sinusitis.
© 2017 Annals of Family Medicine, Inc.
Conflict of interest statement
Conflicts of interest: authors report none.
Figures
References
-
- Wald ER, Applegate KE, Bordley C, et al. ; American Academy of Pediatrics. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics. 2013;132(1):e262–e280. - PubMed
-
- Chow AW, Benninger MS, Brook I, et al. ; Infectious Diseases Society of America. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54(8):e72–e112. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. JAMA. 2016;315(17):1864–1873. - PubMed
-
- Williams JW, Jr, Simel DL. Does this patient have sinusitis? Diagnosing acute sinusitis by history and physical examination. JAMA. 1993;270(10):1242–1246. - PubMed
-
- Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. 2003;56(11):1129–1135. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous