

Magnetic resonance imaging may predict deep remission in patients with perianal fistulizing Crohn's disease
- PMID: 28694669
- PMCID: PMC5483503
- DOI: 10.3748/wjg.v23.i23.4285
Magnetic resonance imaging may predict deep remission in patients with perianal fistulizing Crohn's disease
Abstract
Aim: To evaluate the imaging course of Crohn's disease (CD) patients with perianal fistulas on long-term maintenance anti-tumor necrosis factor (TNF)-α therapy and identify predictors of deep remission.
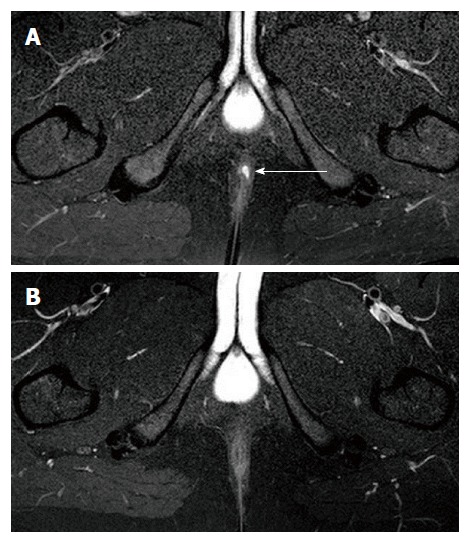
Methods: All patients with perianal CD treated with anti-TNF-α therapy at our tertiary care center were evaluated by magnetic resonance imaging (MRI) and clinical assessment. Two MR examinations were performed: at initiation of anti-TNF-α treatment and then at least 2 years after. Clinical assessment (remission, response and non-response) was based on Present's criteria. Rectoscopic patterns, MRI Van Assche score, and MRI fistula activity signs (T2 signal and contrast enhancement) were collected for the two MR examinations. Fistula healing was defined as the absence of T2 hyperintensity and contrast enhancement on MRI. Deep remission was defined as the association of both clinical remission, absence of anal canal ulcers and healing on MRI. Characteristics and imaging patterns of patients with and without deep remission were compared by univariate and multivariate analyses.
Results: Forty-nine consecutive patients (31 females and 18 males) were included. They ranged in age from 14-70 years (mean, 33 years). MRI and clinical assessment were performed after a mean period of exposure to anti-TNF-α therapy of 40 ± 3.7 mo. Clinical remission, response and non-response were observed in 53.1%, 20.4%, and 26.5% of patients, respectively. Deep remission was observed in 32.7% of patients. Among the 26 patients in clinical remission, 10 had persisting inflammation of fistulas on MRI (T2 hyperintensity, n = 7; contrast enhancement, n = 10). Univariate analysis showed that deep remission was associated with the absence of rectal involvement and the absence of switch of anti-TNF-α treatment or surgery requirement. Multivariate analysis demonstrated that only the absence of rectal involvement (OR = 4.6; 95%CI: 1.03-20.5) was associated with deep remission.
Conclusion: Deep remission is achieved in approximately one third of patients on maintenance anti-TNF-α therapy. Absence of rectal involvement is predictive of deep remission.
Keywords: Anal fistula; Anus disease/diagnosis; Biotherapy; Crohn’s disease; Magnetic resonance imaging.
Conflict of interest statement
Conflict-of-interest statement: There are no conflict of interest to report.
Figures
Similar articles
-
Deep remission on magnetic resonance imaging impacts outcomes of perianal fistulizing Crohn's disease.Dig Liver Dis. 2019 Mar;51(3):358-363. doi: 10.1016/j.dld.2018.12.010. Epub 2018 Dec 23. Dig Liver Dis. 2019. PMID: 30612820
-
Fistulizing perianal Crohn's disease: contrast-enhanced magnetic resonance imaging assessment at 1 year on maintenance anti-TNF-alpha therapy.Inflamm Bowel Dis. 2011 Aug;17(8):1751-8. doi: 10.1002/ibd.21568. Epub 2010 Nov 29. Inflamm Bowel Dis. 2011. PMID: 21744430 Clinical Trial.
-
Long-term MRI-guided combined anti-TNF-α and thiopurine therapy for Crohn's perianal fistulas.Inflamm Bowel Dis. 2012 Oct;18(10):1825-34. doi: 10.1002/ibd.21940. Epub 2012 Jan 4. Inflamm Bowel Dis. 2012. PMID: 22223472
-
Anoperineal lesions in Crohn's disease: French recommendations for clinical practice.Tech Coloproctol. 2017 Sep;21(9):683-691. doi: 10.1007/s10151-017-1684-y. Epub 2017 Sep 19. Tech Coloproctol. 2017. PMID: 28929282 Review.
-
Anti-TNF and fistulizing perianal Crohn's disease: use in clinical practice.Curr Drug Targets. 2010 Feb;11(2):187-97. doi: 10.2174/138945010790309966. Curr Drug Targets. 2010. PMID: 19916954 Review.
Cited by
-
Prognostic factors for the efficacy of infliximab in patients with luminal fistulizing Crohn's disease.BMC Gastroenterol. 2023 Mar 8;23(1):57. doi: 10.1186/s12876-023-02676-9. BMC Gastroenterol. 2023. PMID: 36890451 Free PMC article.
-
Radiological outcomes in perianal fistulizing Crohn's disease: A systematic review and meta-analysis.JGH Open. 2019 Dec 30;4(3):340-344. doi: 10.1002/jgh3.12295. eCollection 2020 Jun. JGH Open. 2019. PMID: 32514434 Free PMC article. Review.
-
Long-term outcomes of perianal fistulizing Crohn's disease in the biologic era.JGH Open. 2020 Dec 20;5(2):235-241. doi: 10.1002/jgh3.12475. eCollection 2021 Feb. JGH Open. 2020. PMID: 33553661 Free PMC article.
-
Total fistula volume predicts surgical outcomes in complex perianal fistulizing Crohn's disease following fistula-tract laser closure: a single-center retrospective study.Tech Coloproctol. 2025 Feb 17;29(1):70. doi: 10.1007/s10151-024-03094-z. Tech Coloproctol. 2025. PMID: 39961900 Free PMC article.
-
Relationship between clinical remission of perianal fistulas in Crohn's disease and serum adalimumab concentrations: A multi-center cross-sectional study.World J Gastroenterol. 2022 Mar 7;28(9):961-972. doi: 10.3748/wjg.v28.i9.961. World J Gastroenterol. 2022. PMID: 35317057 Free PMC article.
References
-
- Chouraki V, Savoye G, Dauchet L, Vernier-Massouille G, Dupas JL, Merle V, Laberenne JE, Salomez JL, Lerebours E, Turck D, et al. The changing pattern of Crohn’s disease incidence in northern France: a continuing increase in the 10- to 19-year-old age bracket (1988-2007) Aliment Pharmacol Ther. 2011;33:1133–1142. - PubMed
-
- Cosnes J, Gower-Rousseau C, Seksik P, Cortot A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology. 2011;140:1785–1794. - PubMed
-
- Schwartz DA, Pemberton JH, Sandborn WJ. Diagnosis and treatment of perianal fistulas in Crohn disease. Ann Intern Med. 2001;135:906–918. - PubMed
-
- Van Assche G, Dignass A, Reinisch W, van der Woude CJ, Sturm A, De Vos M, Guslandi M, Oldenburg B, Dotan I, Marteau P, et al. The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Special situations. J Crohns Colitis. 2010;4:63–101. - PubMed
-
- Rutgeerts P. Review article: treatment of perianal fistulizing Crohn’s disease. Aliment Pharmacol Ther. 2004;20 Suppl 4:106–110. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
