

Rehabilitation after Total Laryngectomy-A Tribute to the Pioneers of Voice Restoration in the Last Two Centuries
- PMID: 28695120
- PMCID: PMC5483444
- DOI: 10.3389/fmed.2017.00081
Rehabilitation after Total Laryngectomy-A Tribute to the Pioneers of Voice Restoration in the Last Two Centuries
Abstract
Background: The most severe consequence of laryngectomy for patients is the loss of their voice. For this reason, voice rehabilitation has been an integral aspect of treatment after total laryngectomy from the very beginning. A wide variety of different technical and surgical approaches are available and reflect the problems associated with the rehabilitation of communication and swallowing after the removal of the larynx.
Methods: We used Internet search engines and libraries to conduct a search of the current medical literature and historical sources of medical information in order to identify and summarize landmark work on this subject.
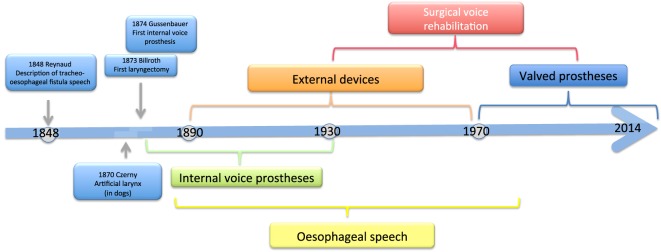
Discussion: Four types of methods have been used to restore the voices of patients, i.e., external devices, esophageal speech, internal voice prostheses, and surgically created tracheo-esophageal fistulas that do not involve the use of a prosthetic device.
Keywords: esophageal speech; laryngeal cancer; total laryngectomy; voice prosthesis; voice rehabilitation.
Figures
References
-
- Maier H, Fischer G, Sennewald E, Heller WD. [Occupational risk factors for pharyngeal cancer. Results of the Heidelberg Pharyngeal Cancer Study]. HNO (1994) 42(9):530–40. - PubMed
-
- Czermak JN. Über die Sprache bei luftdichter Verschließung des Kehlkopfes. Wien Akad Wiss (1859) 35:65–72.
-
- Onodi A. Die künstliche Stimme und Sprache. Monatschr Ohrenheilk Laryngorhinol (1918) 52:85–102.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources