

Prospective quality of life assessment after hip and knee arthroplasty: short- and mid-term follow-up results
- PMID: 28695185
- PMCID: PMC5485233
- DOI: 10.1016/j.artd.2016.09.008
Prospective quality of life assessment after hip and knee arthroplasty: short- and mid-term follow-up results
Abstract
Background: Hip and knee arthroplasty aims to restore the joint function and to improve health-related quality of life (HRQoL) in patients with articular damage. It is important to quantify the HRQoL improvement and when this is achieved. The Oxford knee score and the Oxford hip score were developed to evaluate patients after knee and hip arthroplasty. We sought to evaluate HRQoL changes in the short and mid term following either primary or revision hip and knee arthroplasty.
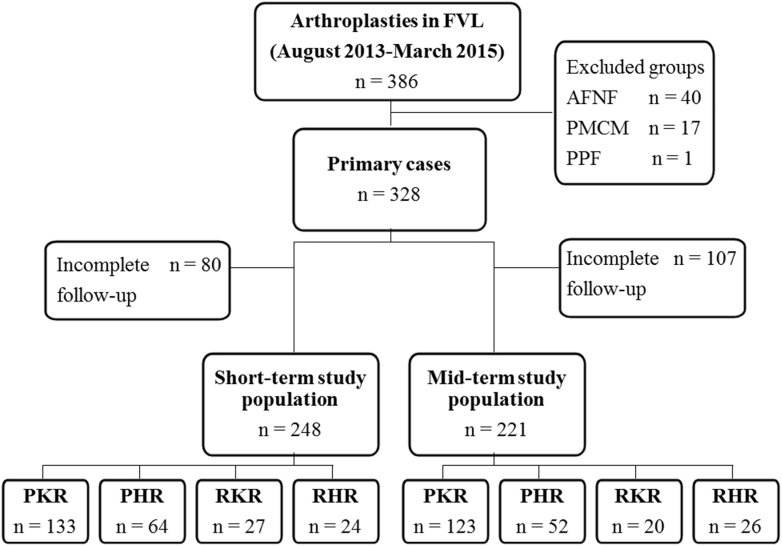
Methods: Prospective cohort study during a 20-month period (August 2013 to March 2015) in a tertiary referral hospital. Primary arthroplasties secondary to osteoarthritis and any-cause revisions were included (328, 160 knees, and 88 hips). They were divided into 4 groups: (1) primary knee replacement, (2) primary hip replacement, (3) revision knee replacement, and (4) revision hip replacement. Oxford knee and hip scores were obtained prior the surgery and compared with the short- and mid-term follow-up scores.
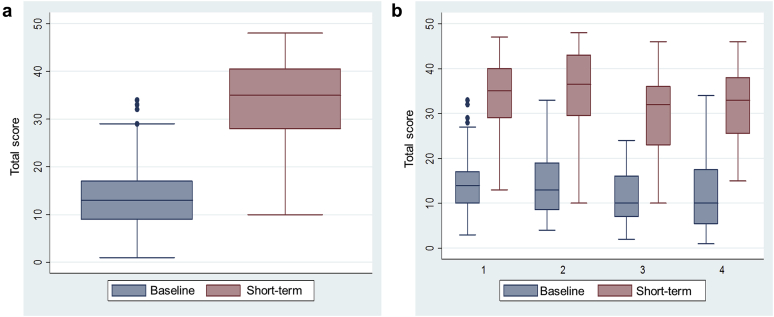
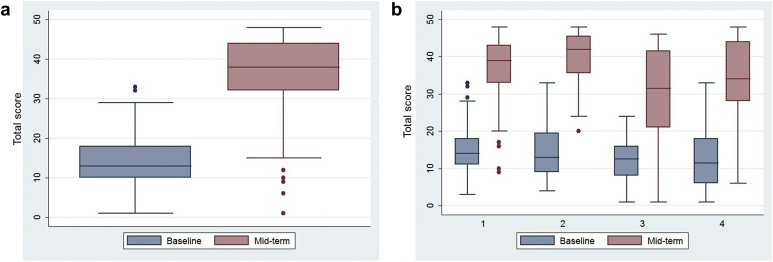
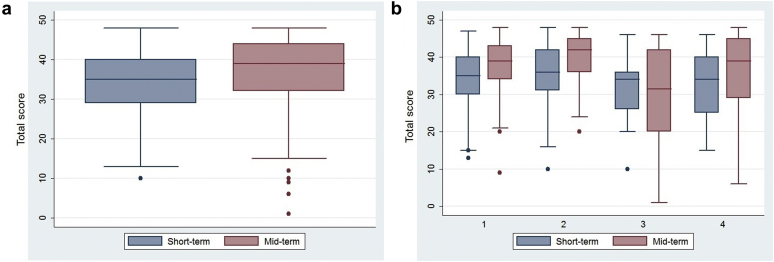
Results: Follow-up in the short term and mid term was: 75.6% and 67.4%, respectively. Improvement was found in both short-term and mid-term follow-up for each group and for the overall group in HRQoL as measured by the Oxford knee and hip scores (P < .001). The greatest improvement was seen in the short term with an increase of 21 points for primary knee arthroplasty; 24 points for primary hip arthroplasty; 22 points for revision knee arthroplasty; and 23 points for revision hip arthroplasty.
Conclusions: Improvement in HRQoL in patients following primary or revision hip or knee arthroplasty is crucial and can be achieved early after the surgery.
Keywords: Hip arthroplasty; Knee arthroplasty; Quality of life.
Figures
References
-
- Ethgen O., Bruyere O., Richy F., Dardennes C., Reginster J.Y. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am. 2004;86-A:963. - PubMed
-
- Jones C.A., Beaupre L.A., Johnston D.W., Suarez-Almazor M.E. Total joint arthroplasties: current concepts of patient outcomes after surgery. Rheum Dis Clin North Am. 2007;33(1):71. - PubMed
-
- Kurtz S., Ong K., Lau E. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780. - PubMed
-
- Liang M.H., Cullen K.E., Larson M.G. Cost-effectiveness of total joint arthroplasty in osteoarthritis. Arthritis Rheum. 1986;29(8):937. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
