

Diagnosis and management of treatment-refractory hypothyroidism: an expert consensus report
- PMID: 28695483
- PMCID: PMC5680379
- DOI: 10.1007/s40618-017-0706-y
Diagnosis and management of treatment-refractory hypothyroidism: an expert consensus report
Abstract
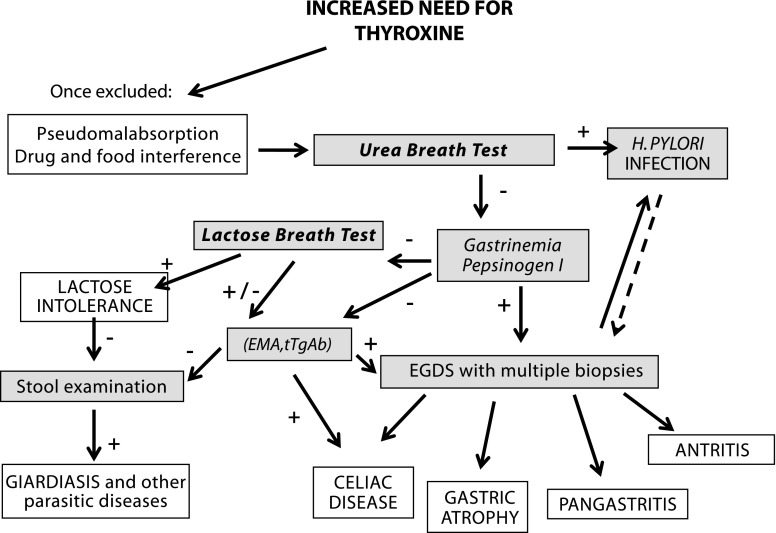
There is a frequently encountered subset of hypothyroid patients who are refractory to standard thyroid hormone replacement treatment and require unexpectedly high doses of levothyroxine. In addition to clinical situations where hypothyroid patients are non-compliant, or where there is the possibility of excipient-induced disease exacerbation (gluten/celiac disease), therapeutic failure may be due to impaired absorption of the administered drug. The common approach to managing patients with unusual thyroxine needs is to escalate the dose of levothyroxine until targeted TSH levels are achieved. This approach can increase the risk for prolonged exposure to supratherapeutic doses of levothyroxine, which increase the chances of adverse outcomes. Repeated adjustments of levothyroxine can also escalate the costs of treatment, as frequent office visits and laboratory tests are required to determine and maintain the desired dose. Clinicians should take a systematic approach to managing patients whom they suspect of having treatment-refractory hypothyroidism. This may include searching for, and adjusting, occult medical conditions and/or other factors that may affect the absorption of levothyroxine, before up-titrating the dose of traditional levothyroxine therapy. Depending on the underlying pathology, another approach that may be considered is to try alternative formulations of levothyroxine that are less susceptible to intolerance issues related to excipients, or, in some cases, to malabsorption. The early discovery of these factors via a thoughtful patient work-up may avoid unnecessary thyroid medication adjustments and their consequences for both patients and clinicians.
Keywords: Hypothyroidism; Levothyroxine; Malabsorption; Refractory.
Conflict of interest statement
Conflict of interest
Marco Centanni, MD, has been a consultant for Akrimax. Dr. Centanni received an honorarium and reimbursement for travel-related expenses from Akrimax for work related to the development of this review. Dr. Centanni has also received honoraria and travel expenses from Akrimax for participation in advisory boards, and from Institut Biochimique SA (IBSA) for attending several international meetings. Salvatore Benvenga, MD, has been a consultant for Akrimax. Dr. Benvenga received an honorarium and reimbursement for travel-related expenses from Akrimax for work related to the development of this review. Dr. Isaac Sachmechi, MD, has been a consultant for Akrimax. Dr. Sachmechi received an honorarium and reimbursement for travel-related expenses from Akrimax for work related to the development of this review. Dr. Sachmechi has received consulting/speaking honoraria from Merck, Novo Nordisk, AstraZeneca, Shire, and Janssen Pharmaceuticals. He has also received study grants from Sanofi-Aventis, Novo Nordisk, AstraZeneca, DermaSciences, Akrimax, and Boehringer Mannheim.
Ethical approval
For this review article, no studies with human participants or animal experimentation were performed by any of the authors.
Informed consent
For this review article, no consent is required.
Figures
Similar articles
-
Diagnosis and treatment of hypothyroidism in TSH deficiency compared to primary thyroid disease: pituitary patients are at risk of under-replacement with levothyroxine.Clin Endocrinol (Oxf). 2011 Jun;74(6):744-9. doi: 10.1111/j.1365-2265.2011.03984.x. Clin Endocrinol (Oxf). 2011. PMID: 21521256
-
Managing Levothyroxine Malabsorption in Refractory Hypothyroidism: A Case Report.Cureus. 2025 Apr 28;17(4):e83123. doi: 10.7759/cureus.83123. eCollection 2025 Apr. Cureus. 2025. PMID: 40438808 Free PMC article.
-
Factors contributing to high levothyroxine doses in primary hypothyroidism: an interventional audit of a large community database.Thyroid. 2014 Dec;24(12):1765-71. doi: 10.1089/thy.2013.0661. Thyroid. 2014. PMID: 25203248
-
Levothyroxine Dose Adjustment to Optimise Therapy Throughout a Patient's Lifetime.Adv Ther. 2019 Sep;36(Suppl 2):30-46. doi: 10.1007/s12325-019-01078-2. Epub 2019 Sep 4. Adv Ther. 2019. PMID: 31485977 Free PMC article. Review.
-
Medication adherence and the use of new pharmaceutical formulations: the case of levothyroxine.Minerva Endocrinol. 2016 Jun;41(2):279-89. Epub 2016 Mar 25. Minerva Endocrinol. 2016. PMID: 27015567 Review.
Cited by
-
Treatment with Intramuscular Levothyroxine in Refractory Hypothyroidism.Eur Thyroid J. 2019 Dec;8(6):319-323. doi: 10.1159/000503324. Epub 2019 Oct 22. Eur Thyroid J. 2019. PMID: 31934558 Free PMC article.
-
Thyroxine Treatment With Softgel Capsule Formulation: Usefulness in Hypothyroid Patients Without Malabsorption.Front Endocrinol (Lausanne). 2018 Mar 21;9:118. doi: 10.3389/fendo.2018.00118. eCollection 2018. Front Endocrinol (Lausanne). 2018. PMID: 29619010 Free PMC article.
-
Macro-Thyrotropin Syndrome: Prevalence and Clinical Profile of an Under-Recognised Rare Entity in Thyroidology.Indian J Endocrinol Metab. 2025 Jan-Feb;29(1):95-100. doi: 10.4103/ijem.ijem_256_24. Epub 2025 Feb 28. Indian J Endocrinol Metab. 2025. PMID: 40181858 Free PMC article.
-
Kisspeptin treatment improves fetal-placental development and blocks placental oxidative damage caused by maternal hypothyroidism in an experimental rat model.Front Endocrinol (Lausanne). 2022 Jul 28;13:908240. doi: 10.3389/fendo.2022.908240. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35966095 Free PMC article.
-
Levothyroxine Therapy in Gastric Malabsorptive Disorders.Front Endocrinol (Lausanne). 2021 Jan 28;11:621616. doi: 10.3389/fendo.2020.621616. eCollection 2020. Front Endocrinol (Lausanne). 2021. PMID: 33584549 Free PMC article. Review.
References
-
- Lips DJ, van Reisen MT, Voigt V, Venekamp W. Diagnosis and treatment of levothyroxine pseudomalabsorption. Neth J Med. 2004;62:114–118. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
