

Contribution of medications and risk factors to QTc interval lengthening in the atherosclerosis risk in communities (ARIC) study
- PMID: 28695724
- PMCID: PMC5741511
- DOI: 10.1111/jep.12776
Contribution of medications and risk factors to QTc interval lengthening in the atherosclerosis risk in communities (ARIC) study
Abstract
Rationale, aims, and objectives: Prolongation of the corrected QT (QTc) interval is associated with increased morbidity and mortality. The association between QTc interval-prolonging medications (QTPMs) and risk factors with magnitude of QTc interval lengthening is unknown. We examined the contribution of risk factors alone and in combination with QTPMs to QTc interval lengthening.
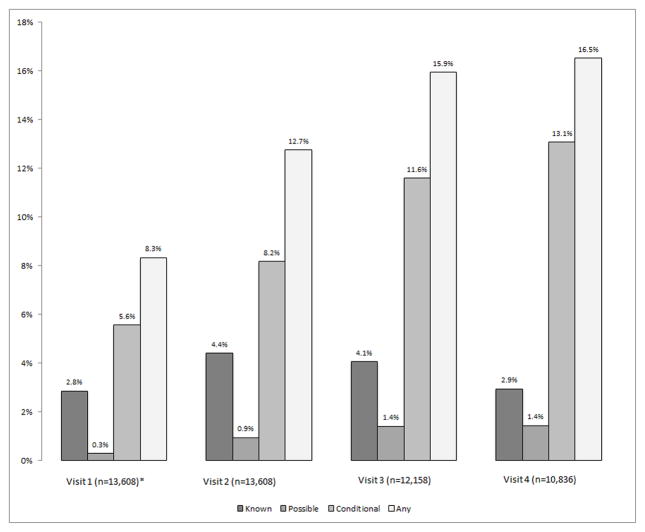
Method: The Atherosclerosis Risk in Communities study assessed 15 792 participants with a resting, standard 12-lead electrocardiogram and ≥1 measure of QTc interval over 4 examinations at 3-year intervals (1987-1998). From 54 638 person-visits, we excluded participants with QRS ≥ 120 milliseconds (n = 2333 person-visits). We corrected the QT interval using the Bazett and Framingham formulas. We examined QTc lengthening using linear regression for 36 602 person-visit observations for 14 160 cohort members controlling for age ≥ 65 years, female sex, left ventricular hypertrophy, QTc > 500 milliseconds at the prior visit, and CredibleMeds categorized QTPMs (Known, Possible, or Conditional risk). We corrected standard errors for repeat observations per person.
Results: Eighty percent of person-visits had at least one risk factor for QTc lengthening. Use of QTPMs increased over the 4 visits from 8% to 17%. Among persons not using QTPMs, history of prolonged QTc interval and female sex were associated with the greatest QTc lengthening, 39 and 12 milliseconds, respectively. In the absence of risk factors, Known QTPMs and ≥2 QTPMs were associated with modest but greater QTc lengthening than Possible or Conditional QTPMs. In the presence of risk factors, ≥2 QTPM further increased QTc lengthening. In combination with risk factors, the association of all QTPM categories with QTc lengthening was greater than QTPMs alone.
Conclusion: Risk factors, particularly female sex and history of prolonged QTc interval, have stronger associations with QTc interval lengthening than any QTPM category alone. All QTPM categories augmented QTc interval lengthening associated with risk factors.
Keywords: QTc interval; QTc prolonging medications; risk factors; torsade de pointes.
© 2017 John Wiley & Sons, Ltd.
Conflict of interest statement
Figures

References
-
- Algra A, Tijssen JG, Roelandt JR, Pool J, Lubsen J. QTc prolongation measured by standard 12-lead electrocardiography is an independent risk factor for sudden death due to cardiac arrest. Circulation. 1991;83(6):1888–1894. - PubMed
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
