

Impact of biliopancreatic limb length on severe protein-calorie malnutrition requiring revisional surgery after one anastomosis (mini) gastric bypass
- PMID: 28695878
- PMCID: PMC5749196
- DOI: 10.4103/jmas.JMAS_198_16
Impact of biliopancreatic limb length on severe protein-calorie malnutrition requiring revisional surgery after one anastomosis (mini) gastric bypass
Abstract
Background: One anastomosis (mini) gastric bypass (OAGB) is believed to be more malabsorptive than Roux-en-Y gastric bypass. A number of patients undergoing this procedure suffer from severe protein-calorie malnutrition requiring revisional surgery. The purpose of this study was to find the magnitude of severe protein-calorie malnutrition requiring revisional surgery after OAGB and any potential relationship with biliopancreatic limb (BPL) length.
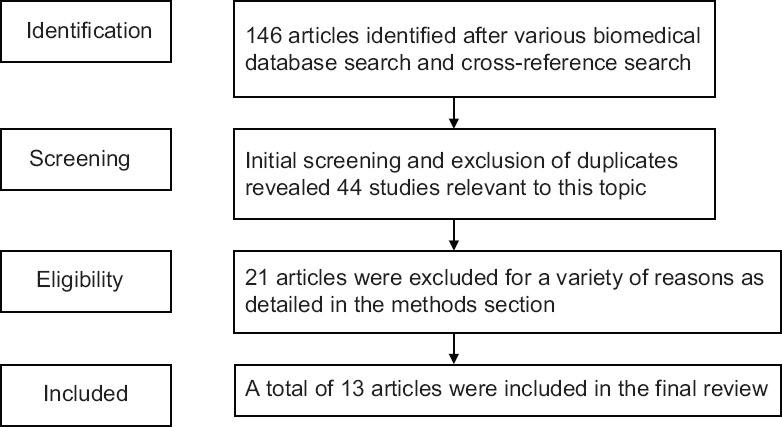
Methods: A questionnaire-based survey was carried out on the surgeons performing OAGB. Data were further corroborated with the published scientific literature.
Results: A total of 118 surgeons from thirty countries reported experience with 47,364 OAGB procedures. Overall, 0.37% (138/36,952) of patients needed revisional surgery for malnutrition. The highest percentage of 0.51% (120/23,277) was recorded with formulae using >200 cm of BPL for some patients, and lowest rate of 0% was seen with 150 cm BPL. These data were corroborated by published scientific literature, which has a record of 50 (0.56%) patients needing surgical revision for severe malnutrition after OAGB.
Conclusions: A very small number of OAGB patients need surgical correction for severe protein-calorie malnutrition. Highest rates of 0.6% were seen in the hands of surgeons using BPL length of >250 cm for some of their patients, and the lowest rate of 0% was seen with BPL of 150 cm. Future studies are needed to examine the efficacy of a standardised BPL length of 150 cm with OAGB.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Mahawar KK, Carr WR, Balupuri S, Small PK. Controversy surrounding ‘mini’ gastric bypass. Obes Surg. 2014;24:324–33. - PubMed
-
- Mahawar KK, Jennings N, Brown J, Gupta A, Balupuri S, Small PK. “Mini” gastric bypass: Systematic review of a controversial procedure. Obes Surg. 2013;23:1890–8. - PubMed
-
- Parmar CD, Mahawar KK, Boyle M, Carr WR, Jennings N, Schroeder N, et al. Mini gastric bypass:First report of 125 consecutive cases from United Kingdom. Clin Obes. 2016;6:61–7. - PubMed
-
- Lee WJ, Ser KH, Lee YC, Tsou JJ, Chen SC, Chen JC. Laparoscopic Roux-en-Y vs.mini-gastric bypass for the treatment of morbid obesity: A 10-year experience. Obes Surg. 2012;22:1827–34. - PubMed
-
- Rutledge R, Walsh TR. Continued excellent results with the mini-gastric bypass: Six-year study in 2,410 patients. Obes Surg. 2005;15:1304–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials