

Impact of pulmonary rehabilitation on postoperative complications in patients with lung cancer and chronic obstructive pulmonary disease
- PMID: 28696575
- PMCID: PMC5582456
- DOI: 10.1111/1759-7714.12466
Impact of pulmonary rehabilitation on postoperative complications in patients with lung cancer and chronic obstructive pulmonary disease
Abstract
Background: Given the extent of the surgical indications for pulmonary lobectomy in breathless patients, preoperative care and evaluation of pulmonary function are increasingly necessary. The aim of this study was to assess the contribution of preoperative pulmonary rehabilitation (PR) for reducing the incidence of postoperative pulmonary complications in non-small cell lung cancer (NSCLC) patients with chronic obstructive pulmonary disease (COPD).
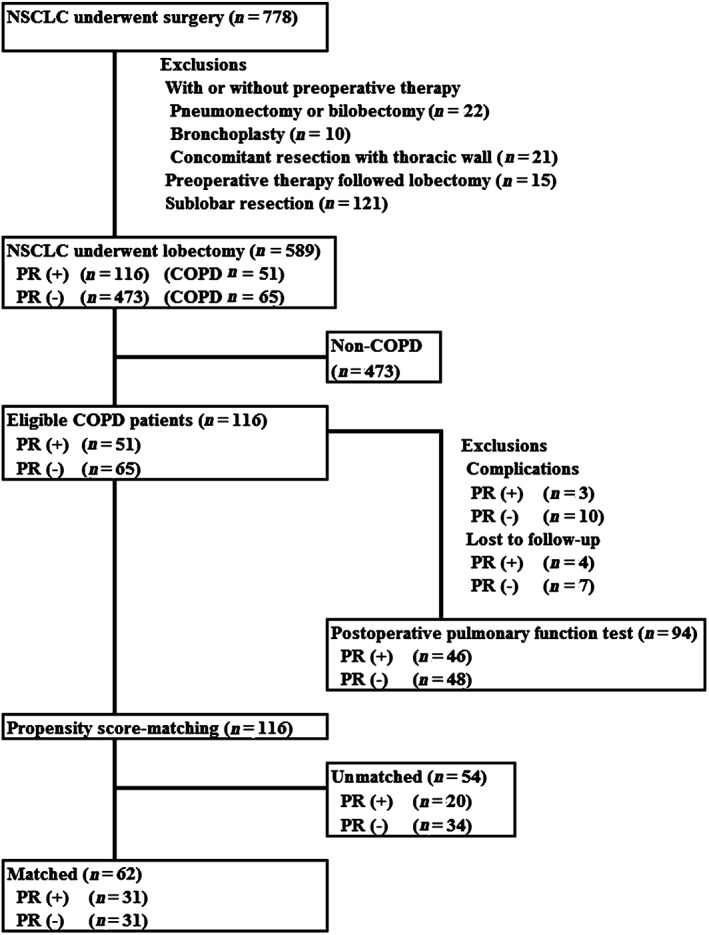
Methods: The records of 116 patients with COPD, including 51 patients who received PR, were retrospectively analyzed. Pulmonary function testing, including slow vital capacity (VC) and forced expiratory volume in one second (FEV1 ), was obtained preoperatively, after PR, and at one and six months postoperatively. The recovery rate of postoperative pulmonary function was standardized for functional loss associated with the different resected lung volumes. Propensity score analysis generated matched pairs of 31 patients divided into PR and non-PR groups.
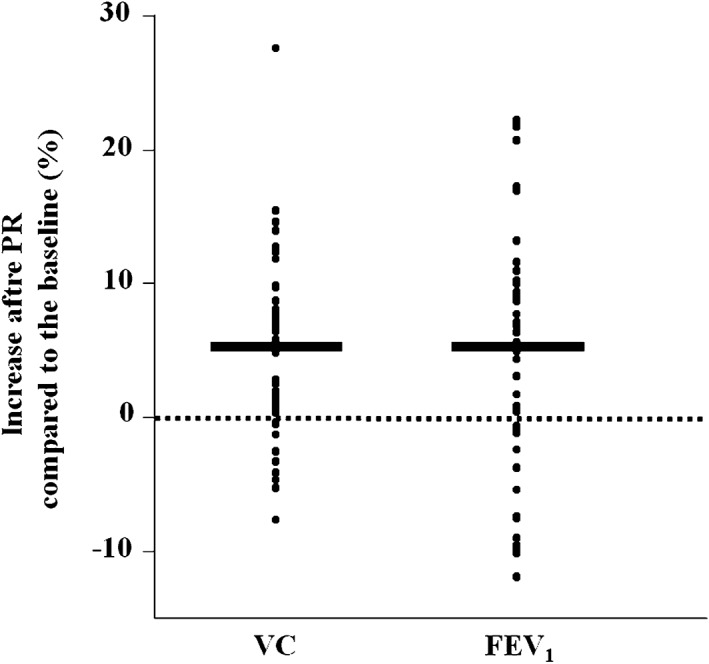
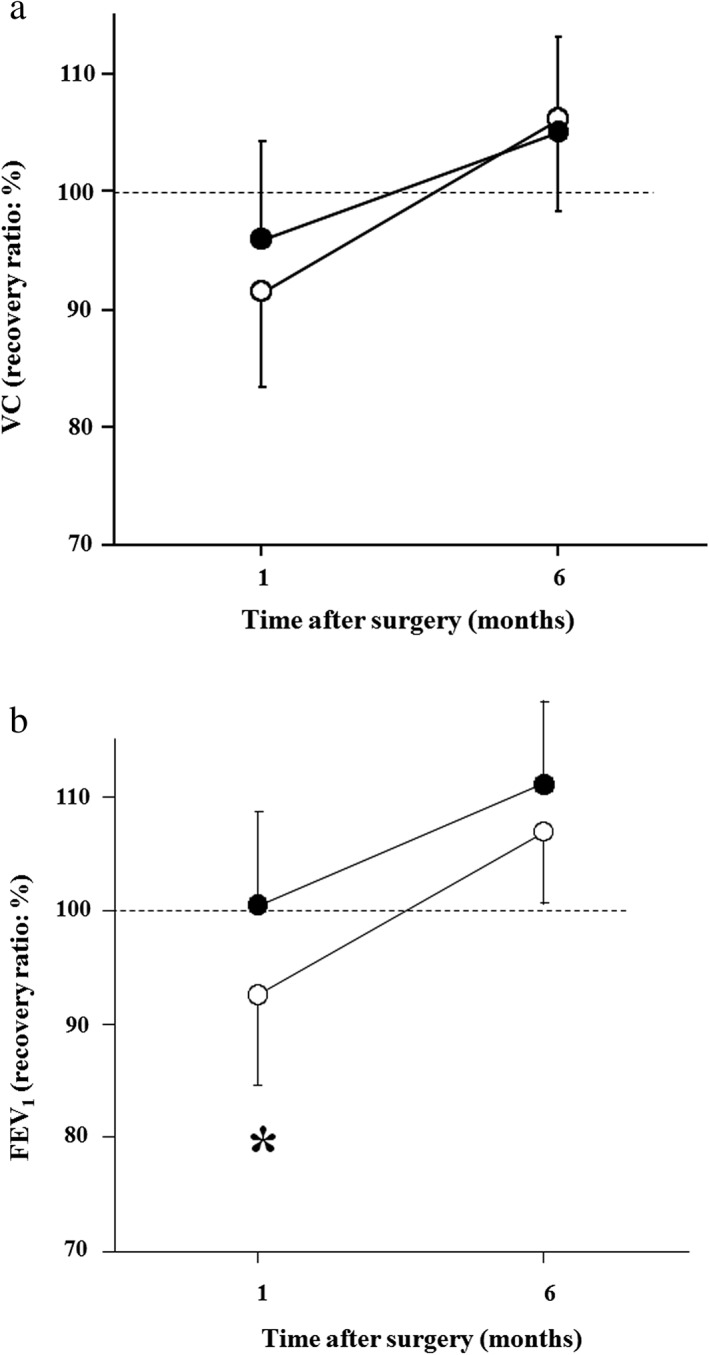
Results: The PR period was 18.7 ± 12.7 days in COPD patients. Preoperative pulmonary function was significantly improved after PR (VC 5.3%, FEV1 5.5%; P < 0.05). The FEV1 recovery rate one month after surgery was significantly better in the PR (101.6%; P < 0.001) than in the non-PR group (93.9%). In logistic regression analysis, predicted postoperative FEV1 , predicted postoperative %FEV1 , and PR were independent factors related to postoperative pulmonary complications after pulmonary lobectomy (odds ratio 18.9, 16.1, and 13.9, respectively; P < 0.05).
Conclusions: PR improved the recovery rate of pulmonary function after lobectomy in the early period, and may decrease postoperative pulmonary complications.
Keywords: Chronic obstructive pulmonary disease; lung cancer; pulmonary rehabilitation.
© 2017 The Authors. Thoracic Cancer published by China Lung Oncology Group and John Wiley & Sons Australia, Ltd.
Figures
References
-
- Licker MJ, Widikker I, Robert J et al. Operative mortality and respiratory complications after lung resection for cancer: Impact of chronic obstructive pulmonary disease and time trends. Ann Thorac Surg 2006; 81: 1830–7. - PubMed
-
- Brunelli A, Kim AW, Berger KI, Addrizzo‐Harris DJ. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence‐based clinical practice guidelines. (Published erratum appears in Chest 2014; 145: 437.). Chest 2013; 143 (5 Suppl.): 166S–90S. - PubMed
-
- Sekine Y, Iwata T, Chiyo M et al. Minimal alteration of pulmonary function after lobectomy in lung cancer patients with chronic obstructive pulmonary disease. Ann Thorac Surg 2003; 76: 356–61. - PubMed
-
- Kushibe K, Takahama M, Tojo T, Kawaguchi T, Kimura M, Taniguchi S. Assessment of pulmonary function after lobectomy for lung cancer‐‐upper lobectomy might have the same effect as lung volume reduction surgery. Eur J Cardiothorac Surg 2006; 29: 886–90. - PubMed
-
- Cooper JD, Trulock EP, Triantafillou AN et al. Bilateral pneumonectomy (volume reduction) for chronic obstructive pulmonary disease. J Thorac Cardiovasc Surg 1995; 109: 106–16. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
