

Transfusion Requirement in Burn Care Evaluation (TRIBE): A Multicenter Randomized Prospective Trial of Blood Transfusion in Major Burn Injury
- PMID: 28697050
- PMCID: PMC5848498
- DOI: 10.1097/SLA.0000000000002408
Transfusion Requirement in Burn Care Evaluation (TRIBE): A Multicenter Randomized Prospective Trial of Blood Transfusion in Major Burn Injury
Abstract
Objective: Our objective was to compare outcomes of a restrictive to a liberal red cell transfusion strategy in 20% or more total body surface area (TBSA) burn patients. We hypothesized that the restrictive group would have less blood stream infection (BSI), organ dysfunction, and mortality.
Background: Patients with major burns have major (>1 blood volume) transfusion requirements. Studies suggest that a restrictive blood transfusion strategy is equivalent to a liberal strategy. However, major burn injury is precluded from these studies. The optimal transfusion strategy in major burn injury is thus needed but remains unknown.
Methods: This prospective randomized multicenter trial block randomized patients to a restrictive (hemoglobin 7-8 g/dL) or liberal (hemoglobin 10-11 g/dL) transfusion strategy throughout hospitalization. Data collected included demographics, infections, transfusions, and outcomes.
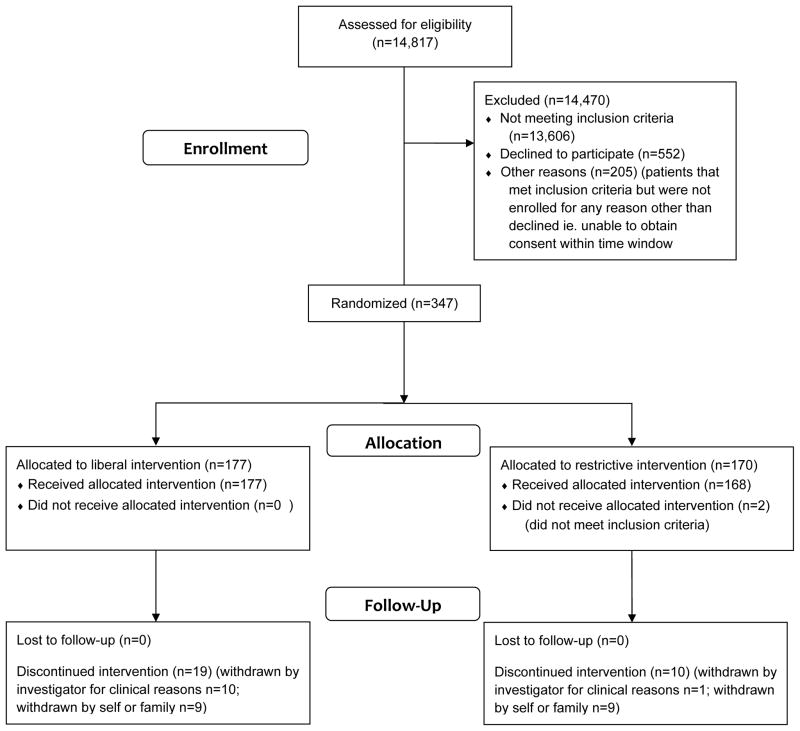
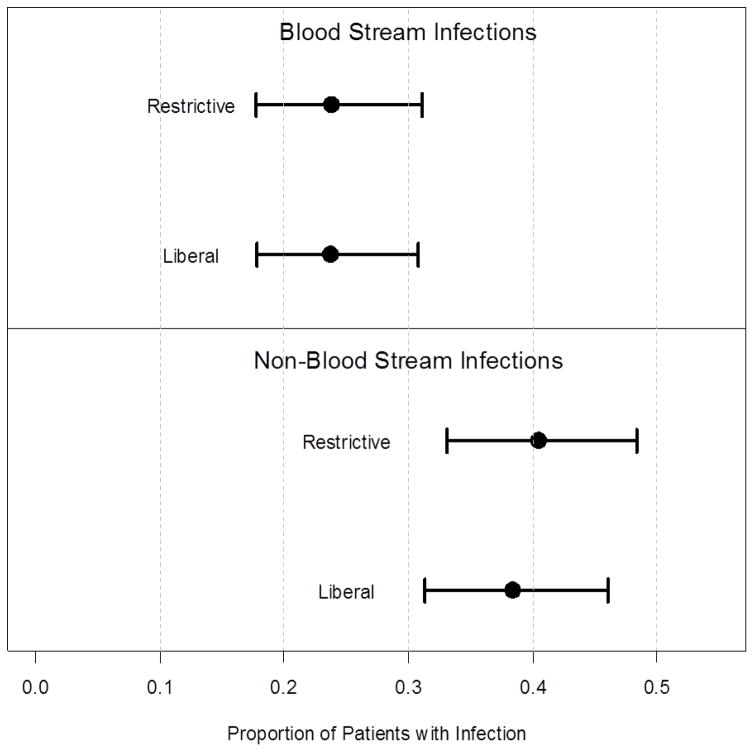
Results: Eighteen burn centers enrolled 345 patients with 20% or more TBSA burn similar in age, TBSA burn, and inhalation injury. A total of 7054 units blood were transfused. The restrictive group received fewer blood transfusions: mean 20.3 ± 32.7 units, median = 8 (interquartile range: 3, 24) versus mean 31.8 ± 44.3 units, median = 16 (interquartile range: 7, 40) in the liberal group (P < 0.0001, Wilcoxon rank sum). BSI incidence, organ dysfunction, ventilator days, and time to wound healing (P > 0.05) were similar. In addition, there was no 30-day mortality difference: 9.5% restrictive versus 8.5% liberal (P = 0.892, χ test).
Conclusions: A restrictive transfusion strategy halved blood product utilization. Although the restrictive strategy did not decrease BSI, mortality, or organ dysfunction in major burn injury, these outcomes were no worse than the liberal strategy (Clinicaltrials.gov identifier NCT01079247).
Conflict of interest statement
Conflicts of Interest and Sources of Funding
Dr. Palmieri: USAMRMC Award #W81XWH-08-1-0760 funded this study
Dr. Holmes: Equity positions in Abbott Labs, AbbVie, and Permeaderm Inc.
Dr. Arnoldo: No conflicts to declare
Dr. Peck: No conflicts to declare
Dr. Potenza: No conflicts to declare
Dr. Cochran: No conflicts to declare
Dr. King: No conflicts to declare
Dr. Dominick: No conflicts to declare
Dr. Cartotto: No conflicts to declare
Dr. Havsar: No conflicts to declare
Dr. Kemalyan: No conflicts to declare
Dr. Tredget: Contract research, Scar X™, KLOX Therapeutics, and Exciton (ExSALT™), collaborative research British Canadian BioSciences Corp (novel antifibrotic agent)
Dr. Stapelberg: No conflicts to declare
Dr. Mozingo: No conflicts to declare
Dr. Friedman: No conflicts to declare
Dr. Greenhalgh: No conflicts to declare
Dr. Taylor: National Center for Research Resources, National Institutes of Health, through grant #UL1 RR024146, the National Center for Advancing Translational Sciences, National Institutes of Health, through grant #TR 000002
Dr. Pollock: No conflicts to declare
Figures
References
-
- Wallace EL, Churchill WH, Surgenor DM, et al. Collection and transfusion of blood and blood components in the United States, 1994. Transfusion. 1998;38:625–636. - PubMed
-
- Hebert PC, Wells G, Martin C, et al. A Canadian survey of transfusion practices in critically ill patients. Crit Care Med. 1998;26:482–487. - PubMed
-
- Marini JJ. Transfusion triggers and Occam’s rusty razor. Crit Care Med. 1998;26:1775–1776. - PubMed
-
- Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409–417. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
