

Implementation of a Risk-Based Heparin Protocol for Postpartum Venous Thromboembolism Prevention
- PMID: 28697098
- PMCID: PMC5529229
- DOI: 10.1097/AOG.0000000000002050
Implementation of a Risk-Based Heparin Protocol for Postpartum Venous Thromboembolism Prevention
Abstract
Objective: To evaluate the effect of a postpartum risk-based low-molecular-weight heparin protocol for venous thromboembolism prevention.
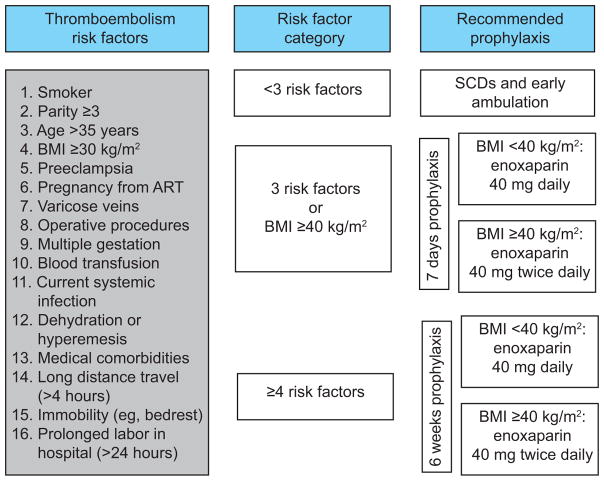
Methods: We conducted a retrospective cohort study of postpartum women at a safety net hospital before (2013), during (2014), and after (2015) implementation of a risk-based enoxaparin thromboembolism prevention protocol. The calculated sample size was based on a primary outcome of enoxaparin administration rate. Secondary outcomes included incidence of postpartum thromboembolism, wound complications, and 30-day readmission rates. The prevalence of thromboembolism risk factors and protocol adherence was evaluated in two groups of women before (May 2013) and after (May 2015) protocol implementation. Exact χ or Cochran-Armitage trend tested differences in rates.
Results: Over 3 years, 9,766 deliveries were included. Enoxaparin was administered to 0.28% (95% CI 0.14-0.55) of postpartum women in 2013 (before) compared with 33.46% (95% CI 31.89-35.07%) after protocol implementation (P<.001). Although underpowered to detect a difference in these outcomes, no differences were seen in rates of thromboembolism (0.16%, 0.12%, 0.15%, P=.9), wound complication (0.82%, 1.21%, 0.91%, P=.7), or emergency department visits (8.30%, 7.96%, 8.34%, P=.9), whereas readmissions increased (0.79%, 1.27%, 1.42%, P=.02). Prevalence of thromboembolism risk factors did not differ between women delivered in May 2013 and May 2015. Physician adherence to the protocol was 89.5% in May 2015. Nine women had thromboembolic events after protocol implementation: five received appropriate treatment per protocol, but four did not. In 2014, three of four women with a thromboembolism were inadequately treated compared with one of five in 2015 with the addition of a computerized order set.
Conclusion: Implementation of a low-molecular-weight heparin risk-based protocol for postpartum thromboembolism prevention resulted in high physician adherence and more than 30% of postpartum women receiving enoxaparin. Before implementing such a protocol on a wider scale, a much larger study is needed to evaluate the effect on thromboembolic disease and wound problems.
Figures
Comment in
-
Patient Safety in Obstetrics: More Evidence, Less Emotion.Obstet Gynecol. 2017 Aug;130(2):257-259. doi: 10.1097/AOG.0000000000002169. Obstet Gynecol. 2017. PMID: 28697095 No abstract available.
References
-
- Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066–74. - PubMed
-
- Royal College of Obstetritians and Gynaecologists. Reducing the Risk of Thrombosis and Embolism During. Green-top Guidel No 37a [Internet] 2009;(37a):1–35. Available from: http://www.rcog.org.uk/files/rcog-corp/GTG37aReducingRiskThrombosis.pdf.
-
- Guimicheva B, Czuprynska J, Arya R. The prevention of pregnancy-related venous thromboembolism. Br J Haematol. 2015;168(2):163–74. - PubMed
-
- D’Alton ME, Friedman AM, Smiley RM, Montgomery DM, Paidas MJ, D’Oria R, et al. National Partnership for Maternal Safety: Consensus Bundle on Venous Thromboembolism. Obstet Gynecol. 2016;128(4):688–98. - PubMed
-
- Barbar S, Noventa F, Rossetto V, Ferrari A, Brandolin B, Perlati M, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: The Padua Prediction Score. J Thromb Haemost. 2010;8(11):2450–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
