

Venous Thromboembolism Prophylaxis During Antepartum Admissions and Postpartum Readmissions
- PMID: 28697100
- PMCID: PMC5598775
- DOI: 10.1097/AOG.0000000000002099
Venous Thromboembolism Prophylaxis During Antepartum Admissions and Postpartum Readmissions
Abstract
Objective: To characterize the use of venous thromboembolism prophylaxis during antepartum and postpartum hospitalizations in the United States.
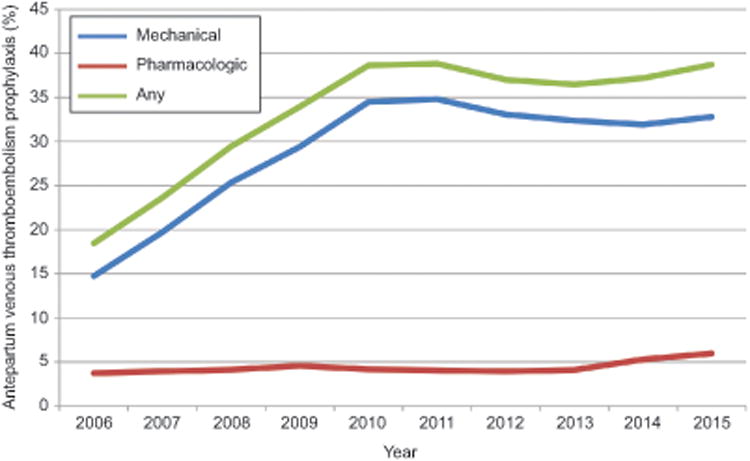
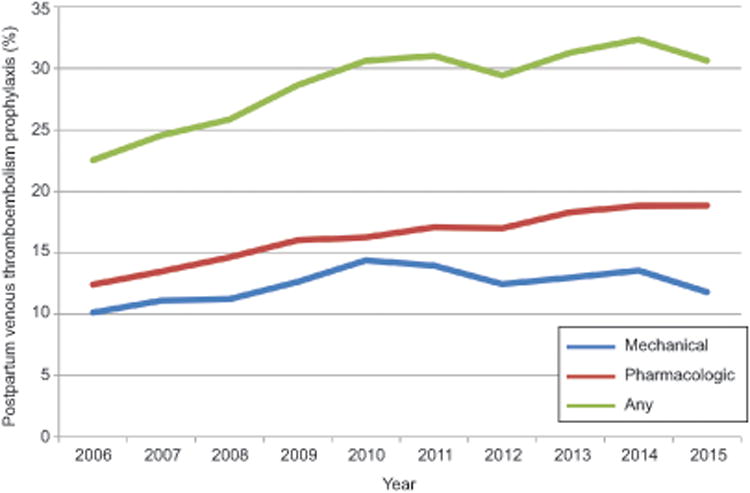
Methods: A retrospective cohort study using the Perspective database was performed to analyze temporal trends of mechanical and pharmacologic venous thromboembolism prophylaxis for patients hospitalized for antepartum and postpartum indications between 2006 and 2015. Delivery hospitalizations were excluded. The association between use of prophylaxis and medical and obstetric risk factors as well as patient demographic and hospital characteristics was evaluated with unadjusted and adjusted models accounting for demographic, hospital and medical, and obstetric risk factors.
Results: A total of 622,740 antepartum and 105,361 postpartum readmissions were identified and included in the analysis. Between 2006 and 2015, use of venous thromboembolism prophylaxis increased from 18.5% to 38.7% for antepartum admissions (adjusted risk ratio [RR] 1.94, 95% CI 1.88-2.01) and from 22.5% to 30.6% for postpartum readmissions (adjusted RR 1.31, 95% CI 1.21-1.43). Among women readmitted postpartum, 56.4% of prophylaxis was pharmacologic and 43.6% was mechanical. For antepartum admissions, 87.2% of prophylaxis was mechanical and 12.8% was pharmacologic. Significant regional and hospital-level variation was noted with prophylaxis most common in the South. In both unadjusted and unadjusted analyses, use of venous thromboembolism prophylaxis was more common for women with thrombophilia, ovarian hyperstimulation syndrome, a history of venous thromboembolism, and prolonged hospitalization. Factors associated with decreased rates of prophylaxis included hyperemesis and postpartum endometritis.
Conclusion: Although antepartum and postpartum venous thromboembolism prophylaxis is becoming increasingly common, particularly in the setting of medical or obstetric risk factors, use of prophylaxis varies regionally and on a hospital level. Some risk factors for venous thromboembolism were associated with lower rates of prophylaxis. The heterogeneity of clinical approaches to venous thromboembolism prophylaxis for these patient populations may represent an opportunity to perform outcomes research to further clarify best practices.
Figures
Comment in
-
Patient Safety in Obstetrics: More Evidence, Less Emotion.Obstet Gynecol. 2017 Aug;130(2):257-259. doi: 10.1097/AOG.0000000000002169. Obstet Gynecol. 2017. PMID: 28697095 No abstract available.
References
-
- Brady MA, Carroll AW, Cheang KI, Straight C, Chelmow D. Sequential compression device compliance in postoperative obstetrics and gynecology patients. Obstet Gynecol. 2015;125:19–25. - PubMed
-
- Creanga AA, Berg CJ, Syverson C, Seed K, Bruce FC, Callaghan WM. Pregnancy-related mortality in the United States, 2006-2010. Obstet Gynecol. 2015;125:5–12. - PubMed
-
- Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ., 3rd Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Annals of internal medicine. 2005;143:697–706. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
