

Contraception After Delivery Among Publicly Insured Women in Texas: Use Compared With Preference
- PMID: 28697112
- PMCID: PMC5563159
- DOI: 10.1097/AOG.0000000000002136
Contraception After Delivery Among Publicly Insured Women in Texas: Use Compared With Preference
Abstract
Objective: To assess women's preferences for contraception after delivery and to compare use with preferences.
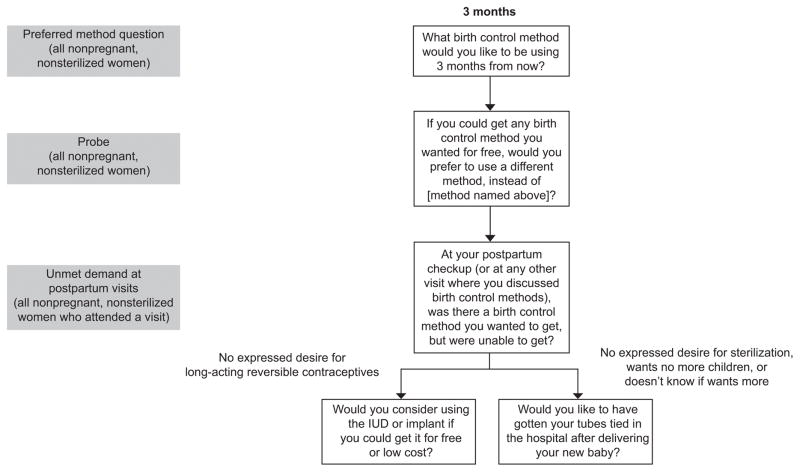
Methods: In a prospective cohort study of women aged 18-44 years who wanted to delay childbearing for at least 2 years, we interviewed 1,700 participants from eight hospitals in Texas immediately postpartum and at 3 and 6 months after delivery. At 3 months, we assessed contraceptive preferences by asking what method women would like to be using at 6 months. We modeled preference for highly effective contraception and use given preference according to childbearing intentions using mixed-effects logistic regression testing for variability across hospitals and differences between those with and without immediate postpartum long-acting reversible contraception (LARC) provision.
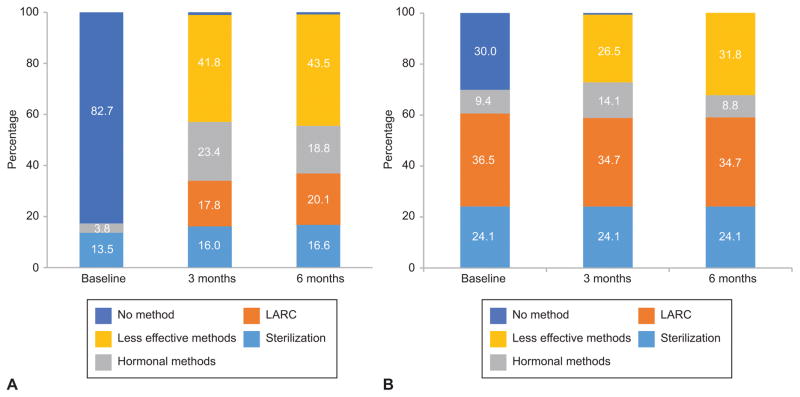
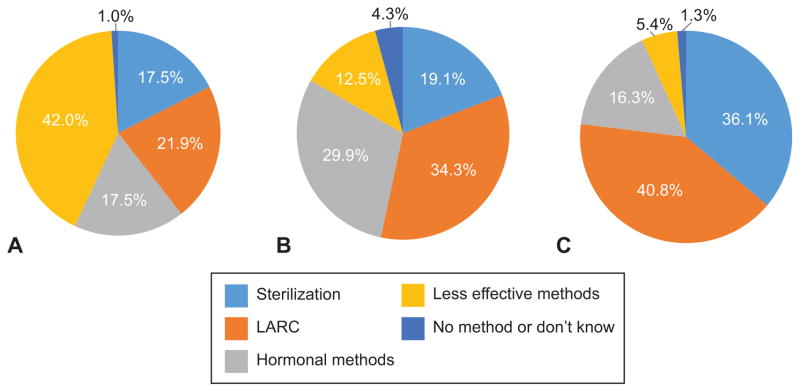
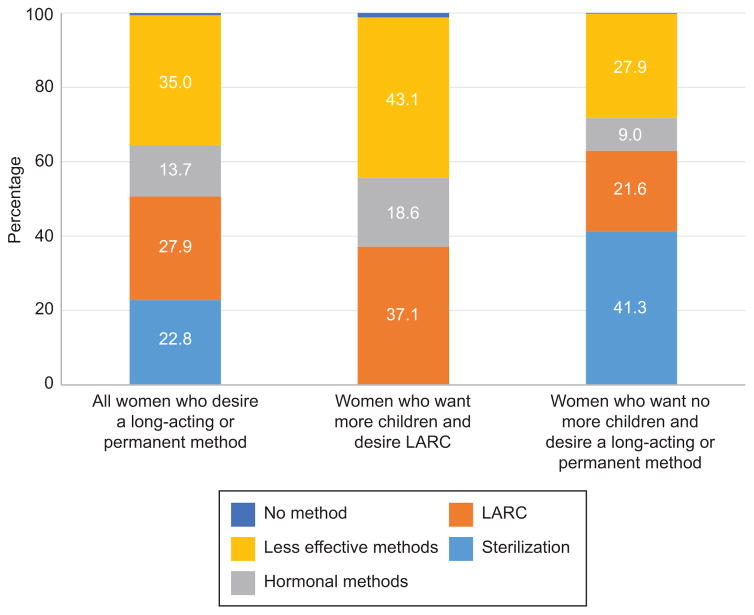
Results: Approximately 80% completed both the 3- and 6-month interviews (1,367/1,700). Overall, preferences exceeded use for both-LARC: 40.8% (n=547) compared with 21.9% (n=293) and sterilization: 36.1% (n=484) compared with 17.5% (n=235). In the mixed-effects logistic regression models, several demographic variables were associated with a preference for LARC among women who wanted more children, but there was no significant variability across hospitals. For women who wanted more children and had a LARC preference, use of LARC was higher in the hospital that offered immediate postpartum provision (P<.035) as it was for U.S.-born women (odds ratio [OR] 2.08, 95% CI 1.17-3.69) and women with public prenatal care providers (OR 2.04, 95% CI 1.13-3.69). In the models for those who wanted no more children, there was no significant variability in preferences for long-acting or permanent methods across hospitals. However, use given preference varied across hospitals (P<.001) and was lower for black women (OR 0.26, 95% CI 0.12-0.55) and higher for U.S.-born women (OR 2.32, 95% CI 1.36-3.96), those 30 years of age and older (OR 1.82, 95% CI 1.07-3.09), and those with public prenatal care providers (OR 2.04, 95% CI 1.18-3.51).
Conclusion: Limited use of long-acting and permanent contraceptive methods after delivery is associated with indicators of health care provider and system-level barriers. Expansion of immediate postpartum LARC provision as well as contraceptive coverage for undocumented women could reduce the gap between preference and use.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
