

Outcomes of subsyndromal delirium in ICU: a systematic review and meta-analysis
- PMID: 28697802
- PMCID: PMC5506578
- DOI: 10.1186/s13054-017-1765-3
Outcomes of subsyndromal delirium in ICU: a systematic review and meta-analysis
Abstract
Background: Subsyndromal delirium (SSD) is a frequent condition and has been commonly described as an intermediate stage between delirium and normal cognition. However, the true frequency of SSD and its impact on clinically relevant outcomes in the intensive care unit (ICU) remains unclear.
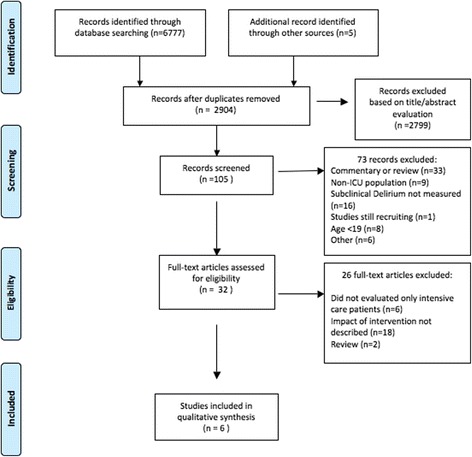
Methods: We performed a systematic search in PubMed, Embase, CINAHL, Cochrane Library, and PsychINFO, with no language restrictions, up to 1 October 2016 to identify publications that evaluated SSD in ICU patients.
Results: The six eligible studies were evaluated. SSD was present in 950 (36%) patients. Four studies evaluated only surgical patients. Four studies used the Intensive Care Delirium Screening Checklist (ICDSC) and two used the Confusion Assessment Method (CAM) score to diagnose SSD. The meta-analysis showed an increased hospital length of stay (LOS) in SSD patients (0.31, 0.12-0.51, p = 0.002; I 2 = 34%). Hospital mortality was described in two studies but it was not significant (hazard ratio 0.97, 0.61-1.55, p = 0.90 and 5% vs 9%, p = 0.05). The use of antipsychotics in SSD patients to prevent delirium was evaluated in two studies but it did not modify ICU LOS (6.5 (4-8) vs 7 (4-9) days, p = 0.66 and 2 (2-3) vs 3 (2-3) days, p = 0.517) or mortality (9 (26.5%) vs 7 (20.6%), p = 0.55).
Conclusions: SSD occurs in one-third of the ICU patients and has limited impact on the outcomes. The current literature concerning SSD is composed of small-sample studies with methodological differences, impairing a clear conclusion about the association between SSD and progression to delirium or worse ICU clinical outcomes.
Keywords: Critically ill; Delirium; ICU; Subsyndromal delirium.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- American Psychiatric Association . Task Force on DSM-V. Diagnostic and statistical manual of mental disorders. 5. Arlington: American Psychiatric Association; 2013. p. 947.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
