

Spirometry, Static Lung Volumes, and Diffusing Capacity
- PMID: 28698266
- PMCID: PMC6373859
- DOI: 10.4187/respcare.05515
Spirometry, Static Lung Volumes, and Diffusing Capacity
Abstract
Background: Spirometric Z-scores from the Global Lung Initiative (GLI) rigorously account for age-related changes in lung function and are thus age-appropriate when establishing spirometric impairments, including a restrictive pattern and air-flow obstruction. However, GLI-defined spirometric impairments have not yet been evaluated regarding associations with static lung volumes (total lung capacity [TLC], functional residual capacity [FRC], and residual volume [RV]) and gas exchange (diffusing capacity).
Methods: We performed a retrospective review of pulmonary function tests in subjects ≥40 y old (mean age 64.6 y), including pre-bronchodilator measures for: spirometry (n = 2,586), static lung volumes by helium dilution with inspiratory capacity maneuver (n = 2,586), and hemoglobin-adjusted single-breath diffusing capacity (n = 2,508). Using multivariable linear regression, adjusted least-squares means (adjLSMeans) were calculated for TLC, FRC, RV, and hemoglobin-adjusted single-breath diffusing capacity. The adjLSMeans were expressed with and without height-cubed standardization and stratified by GLI-defined spirometry, including normal (n = 1,251), restrictive pattern (n = 663), and air-flow obstruction (mild, [n = 128]; moderate, [n = 150]; and severe, [n = 394]).
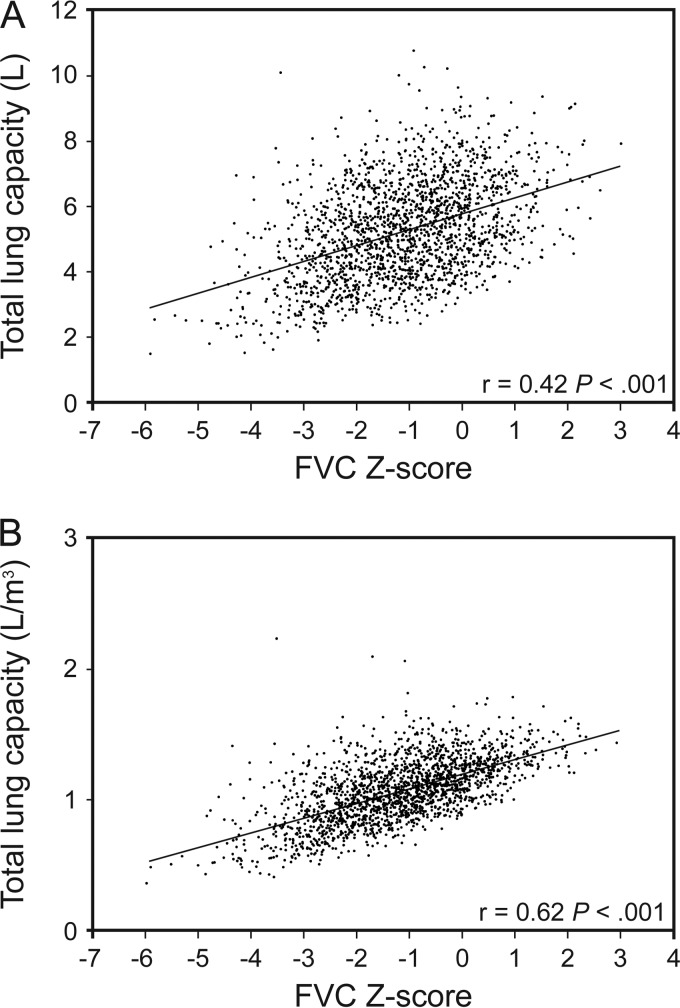
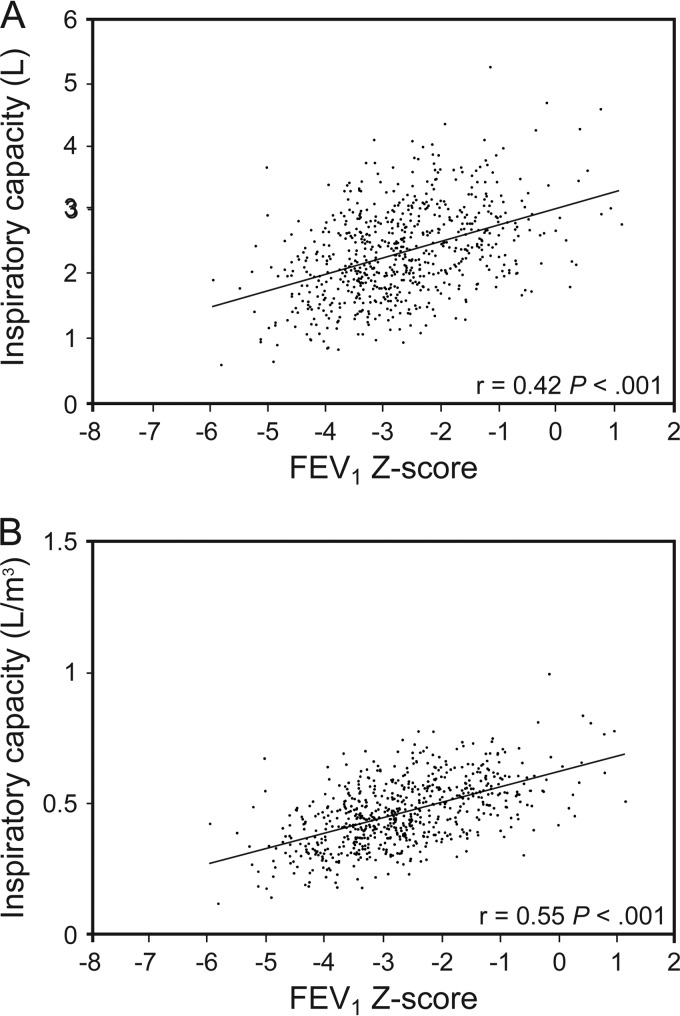
Results: Relative to normal spirometry, restrictive-pattern had lower adjLSMeans for TLC, FRC, RV, and hemoglobin-adjusted single-breath diffusing capacity (P ≤ .001). Conversely, relative to normal spirometry, mild, moderate, and severe air-flow obstruction had higher adjLSMeans for FRC and RV (P < .001). However, only mild and moderate air-flow obstruction had higher adjLSMeans for TLC (P < .001), while only moderate and severe air-flow obstruction had higher adjLSMeans for RV/TLC (P < .001) and lower adjLSMeans for hemoglobin-adjusted single-breath diffusing capacity (P < .001). Notably, TLC (calculated as FRC + inspiratory capacity) was not increased in severe air-flow obstruction (P ≥ .11) because inspiratory capacity decreased with increasing air-flow obstruction (P < .001), thus opposing the increased FRC (P < .001). Finally, P values were similar whether adjLSMeans were height-cubed standardized.
Conclusions: A GLI-defined spirometric restrictive pattern is strongly associated with a restrictive ventilatory defect (decreased TLC, FRC, and RV), while GLI-defined spirometric air-flow obstruction is strongly associated with hyperinflation (increased FRC) and air trapping (increased RV and RV/TLC). Both spirometric impairments were strongly associated with impaired gas exchange (decreased hemoglobin-adjusted single-breath diffusing capacity).
Keywords: Global Lung Initiative; air trapping; diffusing capacity; hyperinflation; restriction; spirometry; static lung volumes.
Copyright © 2017 by Daedalus Enterprises.
Conflict of interest statement
The authors have disclosed no conflicts of interest.
Figures
Comment in
-
Does Global Lung Initiative Obviate the Need for Lung Volume Measurements?Respir Care. 2017 Sep;62(9):1228-1229. doi: 10.4187/respcare.05831. Respir Care. 2017. PMID: 28830988 No abstract available.
Similar articles
-
Diffusing capacity in normal-for-age spirometry and spirometric impairments, using reference equations from the global lung function initiative.Respir Med. 2020 Aug-Sep;170:106037. doi: 10.1016/j.rmed.2020.106037. Epub 2020 May 21. Respir Med. 2020. PMID: 32843169 Free PMC article.
-
Restrictive impairment in patients with asthma.Respir Med. 2007 Feb;101(2):272-6. doi: 10.1016/j.rmed.2006.05.008. Epub 2006 Jun 22. Respir Med. 2007. PMID: 16797172
-
What is the clinical value of lung volumes?Respir Care. 2012 Jan;57(1):26-35; discussion 35-8. doi: 10.4187/respcare.01374. Respir Care. 2012. PMID: 22222123
-
On the causes of lung hyperinflation during bronchoconstriction.Eur Respir J. 1997 Feb;10(2):468-75. doi: 10.1183/09031936.97.10020468. Eur Respir J. 1997. PMID: 9042651 Review.
-
Body plethysmography--its principles and clinical use.Respir Med. 2011 Jul;105(7):959-71. doi: 10.1016/j.rmed.2011.02.006. Epub 2011 Feb 26. Respir Med. 2011. PMID: 21356587 Review.
Cited by
-
Diffusing capacity in normal-for-age spirometry and spirometric impairments, using reference equations from the global lung function initiative.Respir Med. 2020 Aug-Sep;170:106037. doi: 10.1016/j.rmed.2020.106037. Epub 2020 May 21. Respir Med. 2020. PMID: 32843169 Free PMC article.
-
Spirometric Criteria for Chronic Obstructive Pulmonary Disease in Clinical Trials of Pharmacotherapy.COPD. 2018 Feb;15(1):17-20. doi: 10.1080/15412555.2018.1424815. COPD. 2018. PMID: 29469677 Free PMC article.
-
Is there a correlation between the changes in airway inflammation and the changes in respiratory mechanics after vaping in patients with asthma?World J Methodol. 2024 Jun 20;14(2):89284. doi: 10.5662/wjm.v14.i2.89284. eCollection 2024 Jun 20. World J Methodol. 2024. PMID: 38983659 Free PMC article. Clinical Trial.
-
Re-evaluation of combination therapy in chronic obstructive pulmonary disease (COPD).Respir Med. 2019 May;151:27-34. doi: 10.1016/j.rmed.2019.03.020. Epub 2019 Mar 29. Respir Med. 2019. PMID: 31047114 Free PMC article.
-
Investigating the relationships among lung function variables in chronic obstructive pulmonary disease in men.PeerJ. 2019 Oct 1;7:e7829. doi: 10.7717/peerj.7829. eCollection 2019. PeerJ. 2019. PMID: 31592356 Free PMC article.
References
-
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26(5):948–968. - PubMed
-
- Aaron SD, Dales RE, Cardinal P. How accurate is spirometry at predicting restrictive pulmonary impairment? Chest 1999;115(3):869–873. - PubMed
-
- Glady CA, Aaron SD, Lunau M, Clinch J, Dales RE. A spirometry-based algorithm to direct lung function testing in the pulmonary function laboratory. Chest 2003;123(6):1939–1946. - PubMed
-
- Crapo RO, Morris AH, Gardner RM. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am Rev Respir Dis 1981;123(6):659–664. - PubMed
-
- Knudson R, Lebowitz M, Holberg C, Burrows B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am Rev Respir Dis 1983;127(6):725–734. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
