

The involvement of physician assistants in inpatient care in hospitals in the Netherlands: a cost-effectiveness analysis
- PMID: 28698344
- PMCID: PMC5541617
- DOI: 10.1136/bmjopen-2017-016405
The involvement of physician assistants in inpatient care in hospitals in the Netherlands: a cost-effectiveness analysis
Abstract
Objective: To investigate the cost-effectiveness of substitution of inpatient care from medical doctors (MDs) to physician assistants (PAs).
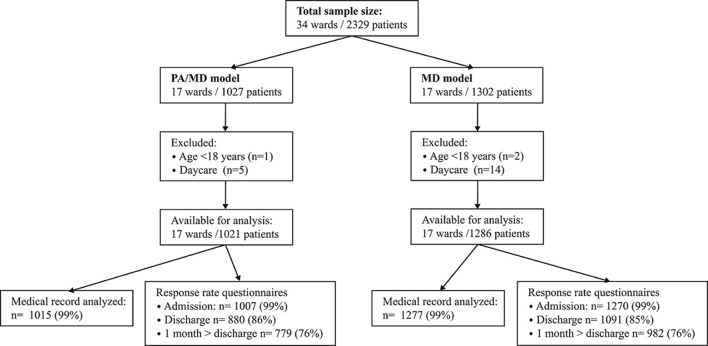
Design: Cost-effectiveness analysis embedded within a multicentre, matched-controlled study. The traditional model in which only MDs are employed for inpatient care (MD model) was compared with a mixed model in which, besides MDs, PAs are also employed (PA/MD model).
Setting: 34 hospital wards across the Netherlands.
Participants: 2292 patients were followed from admission until 1 month after discharge. Patients receiving daycare, terminally ill patients and children were excluded.
Primary and secondary outcome measures: All direct healthcare costs from day of admission until 1 month after discharge. Health outcome concerned quality-adjusted life years (QALYs), which was measured with the EuroQol five dimensions questionnaire (EQ-5D).
Results: We found no significant difference for QALY gain (+0.02, 95% CI -0.01 to 0.05) when comparing the PA/MD model with the MD model. Total costs per patient did not significantly differ between the groups (+€568, 95% CI -€254 to €1391, p=0.175). Regarding the costs per item, a difference of €309 per patient (95% CI €29 to €588, p=0.030) was found in favour of the MD model regarding length of stay. Personnel costs per patient for the provider who is primarily responsible for medical care on the ward were lower on the wards in the PA/MD model (-€11, 95% CI -€16 to -€6, p<0.01).
Conclusions: This study suggests that the cost-effectiveness on wards managed by PAs, in collaboration with MDs, is similar to the care on wards with traditional house staffing. The involvement of PAs may reduce personnel costs, but not overall healthcare costs.
Trial registration number: NCT01835444.
Keywords: Professional role revision; costs; hospital care; physician assistant; resource use; substitution.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Cawley JF, Hooker RS. Physician assistants in American medicine: the half-century mark. Am J Manag Care 2013;19:e333–41. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous